- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Laparoscopy

UPMC liver surgeons are among the most experienced in the world in performing minimally invasive liver surgery. Most patients benefit from less trauma and pain, minimal scarring, a shorter hospital stay, and faster recovery than from traditional surgery.
To learn more, please visit https://www.upmc.com/services/....liver-cancer/treatme

Dr. Lohith U, Consultant Surgical Gastroenterology, Bariatric and GI Oncology, Manipal Hospital Sarjapur, speaks about advanced laparoscopic surgery in this informative video. He shares details about the procedure,insights on its advantages, and how it can help treat gastrointestinal issues without making large incisions in a patient’s body. To know more watch this video.
Consult the experts here - https://bit.ly/3RiWqPr
#ManipalHospitalSarjapur #YourManipal #LifesOn #Healthcare #LaparoscopicSurgery


This video demonstrates Laparoscopic Cholecystectomy Fully Explained Skin-to-Skin Video with Near Infrared Cholangiography performed by Dr R K Mishra at World Laparoscopy Hospital. A laparoscopic cholecystectomy is a minimally invasive surgical procedure that involves removing the gallbladder. It is typically performed using small incisions in the abdomen, through which a laparoscope (a thin tube with a camera and light) and surgical instruments are inserted. The surgeon uses the laparoscope to visualize the inside of the abdomen and to guide the instruments in removing the gallbladder.
Near-infrared cholangiography is a technique that uses a special camera and fluorescent dye to visualize the bile ducts during surgery. The dye is injected into the cystic duct (the tube that connects the gallbladder to the bile ducts) and the camera detects the fluorescence emitted by the dye, allowing the surgeon to see the bile ducts more clearly.
The combination of laparoscopic cholecystectomy and near-infrared cholangiography has become a standard of care in many hospitals and surgical centers. It allows for a more precise and efficient surgery, reducing the risk of complications such as bile duct injury.
The use of indocyanine green (ICG) with near-infrared imaging during laparoscopic cholecystectomy has several advantages. Here are some of them:
Better visualization of the biliary anatomy: ICG with near-infrared imaging allows for better visualization of the biliary anatomy during surgery. This helps the surgeon identify important structures, such as the cystic duct and the common bile duct, and avoid injuring them.
Reduced risk of bile duct injury: With better visualization of the biliary anatomy, the risk of bile duct injury during surgery is reduced. Bile duct injury is a serious complication that can occur during laparoscopic cholecystectomy and can lead to long-term health problems.
Improved surgical precision: ICG with near-infrared imaging also improves surgical precision. The surgeon can better see the tissues and structures being operated on, which can help reduce the risk of bleeding and other complications.
Shorter operating time: The use of ICG with near-infrared imaging can shorten the operating time for laparoscopic cholecystectomy. This is because the surgeon can more quickly and accurately identify the biliary anatomy, which can help streamline the surgery.
Overall, the use of ICG with near-infrared imaging is a valuable tool in laparoscopic cholecystectomy that can improve surgical outcomes and reduce the risk of complications.
Like any surgical procedure, laparoscopic cholecystectomy (gallbladder removal) has potential complications. Here are some of the most common ones:
Bleeding: Bleeding during or after the surgery is a possible complication of laparoscopic cholecystectomy. Most cases are minor and can be easily controlled, but in rare cases, significant bleeding may require a blood transfusion or even additional surgery.
Infection: Any surgical procedure carries a risk of infection. After laparoscopic cholecystectomy, there is a risk of infection at the site of the incisions or within the abdomen. Symptoms may include fever, pain, redness, or drainage from the incision sites.
Bile leakage: In some cases, a small amount of bile may leak from the bile ducts into the abdominal cavity after gallbladder removal. This can cause abdominal pain, fever, and sometimes requires further surgery or treatment.
Injury to nearby organs: During the surgery, there is a small risk of unintentional injury to nearby organs such as the liver, intestines, or bile ducts. This can cause additional complications and may require further treatment.
Adverse reactions to anesthesia: As with any surgery requiring general anesthesia, there is a small risk of adverse reactions to the anesthesia, such as an allergic reaction, respiratory problems, or heart complications.
Most patients recover without complications following a laparoscopic cholecystectomy, but it is important to discuss any concerns or questions with your surgeon beforehand.
Contact us
World Laparoscopy Hospital
Cyber City, Gurugram, NCR Delhi
INDIA : +919811416838
World Laparoscopy Training Institute
Bld.No: 27, DHCC, Dubai
UAE : +971525857874
World Laparoscopy Training Institute
8320 Inv Dr, Tallahassee, Florida
USA : +1 321 250 7653
Regenerate response

Unique 3D technology from Olympus:
http://www.olympus-europa.com/....medical/en/medical_s
Discover the 3rd dimension of endoscopy and experience laparoscopy in a totally new dimension.
Contact us for more information:http://www.olympus-europa.com/....medical/en/medical_s

This video demonstrate Bilateral Salpingectomy for a patient suffering from hematosalpinx of one side and Hydrosalpinx other side in which one IVF has failed. Laparoscopic salpingectomy. In this less-invasive procedure, the surgeon makes 1-3 small incisions in the lower abdomen, and inserts a laparoscope into the pelvis through one of the incisions. The camera at the end of the laparoscope guides the surgeon through the procedure. The fallopian tube tissue is then removed. For more information https://www.laparoscopyhospital.com/
For more information please contact:
World Laparoscopy Hospital
Cyber City, Gurugram, NCR DELHI
INDIA 122002
Phone & WhatsApp: +919811416838, + 91 9999677788

Colorectal surgeon Conor Delaney, MD, explains laparoscopic surgery for colon cancer, including how it works and what patients can typically expect before, during, and after the procedure.
Learn more about colon cancer at http://cancer.org/coloncancer

For more videos, please visit:
http://surgicalfilmatlas.mssm.edu/

Product demonstration video for the Cardinal Health™ Laparoscopic Abdominal Drape (cat. no. 9438)

http://drraewynteirney.com.au/video/
http://drraewynteirney.com.au/....about-dr-raewyn-teir
Dr Raewyn Teirney - fertility specialist and Gynaecologist in Sydney shows a video recording of a laparoscopy for a woman with infertility and pelvic pain.

VirtaMed's new laparoscopy simulator starts with patient safety.
VirtaMed LaparoS™
-Starts at the beginning and covers crucial procedure preparation steps
- Innovative skills training derived from validated concepts
- Start with patient safety: abdomen positioning and trocar placement
- Covers crucial procedure preparation steps
Numerous medical training institutions have found that integrating simulation into their curriculum both improves training outcomes and ultimately supports better patient care. Benefit from VirtaMed’s decades of experience and expertise in laparoscopy training and education.

This video demonstrate Laparoscopic Cholecystectomy Full Length Skin to Skin Video with Infrared Cholangiography performed by Dr R K Mishra at World Laparoscopy Hospital. Infrared Cholegiography is performed by using Indocyanine Green during laparoscopic cholecystectomy surgery for gallbladder removal. Bile duct injury remains the most feared complication of laparoscopic cholecystectomy. Intraoperative cholangiography (IOC) is the current gold standard for biliary imaging and may reduce injury, but is not widely used because of the difficulties of doing it. Near-Infrared Fluorescence Cholangiography (NIRF-C) is a novel non-invasive method for real-time, radiation-free, intra-operative biliary mapping during laparoscopic cholecystectomy. We have experienced that NIRF-C is a safe and effective method for identifying biliary anatomy during laparoscopic cholecystectomy. Indocyanine green is a cyanine dye is very popular and used for many years in medical diagnostics. It is used for determining cardiac output, hepatic function, liver, and gastric blood flow, and for ophthalmic angiography. Now the use of this dye in lap chole has improved the safety of this surgery by NEAR INFRARED FLUORESCENT CHOLANGIOGRAPHY.
For more information please contact:
World Laparoscopy Hospital
Cyber City, Gurugram, NCR DELHI
INDIA 122002
Phone & WhatsApp: +919811416838, + 91 9999677788

Vatche, Minassian, MD, MPH, Chief of Urogynecology, and Sarah Cohen, MD, MPH, Director of the Minimally Invasive Gynecologic Surgery Fellowship Program at Brigham and Women’s Hospital, perform a laparoscopic burch colposuspension, a procedure used to correct stress urinary incontinence.
Stress urinary incontinence is one of the most common types of incontinence and is characterized by urinary leakage during physical activities including coughing, sneezing, exercising, lifting, and laughing. As the condition progresses, it can become severe enough to happen with simple acts such as bending and walking. This condition is due to an anatomic weakness of the bladder neck which typically maintains the seal of urine during activity. Stress incontinence can result from a variety of conditions including vaginal childbirth, aging, menopause and obesity. As this is an anatomic condition, primary treatment may involve pelvic floor exercises and/or minimally invasive surgery.
Learn more about treatment for stress urinary incontinence:
Division of Urogynecology: http://www.brighamandwomens.or....g/Departments_and_Se
Division of Minimally Invasive Gynecologic Surgery: http://www.brighamandwomens.or....g/Departments_and_Se

Laparoscopic surgery is minimally-invasive (keyhole) surgery and it is performed through very small incisions, using a camera to guide the surgeon during the procedure. Miss Sarah Mills, a top colorectal surgeon, explains why laparoscopic surgery is performed over alternative methods.
Make an appointment with Miss Sarah Mills here: https://www.topdoctors.co.uk/doctor/sarah-mills

Sean Langenfeld, M.D., UNMC College of Medicine

UPDATE 1/30/15: Watch the updated version of this animation: https://www.youtube.com/watch?v=LVP6JngpgEE
This 3D medical animation shows how adhesions in the abdomen may cause complications. These problems may include obstruction, twisting, and dislocating areas of the small intestine. Adhesions can be separated with laparoscopic instruments.
ANH00037

UPDATE 2/6/15: A new version of this animation is now available! https://www.youtube.com/watch?v=E1ljClS0DhM
This 3D medical animation depicts the surgical removal of the appendix (appendectomy) using laparoscopic instruments. The surgery animation begins by showing an inflamed appendix (appendicitis), followed by the placement of the laparoscope. Afterward, one can see the surgical device staple, cut and remove the inflamed appendix. Following the removal of the appendix the abdomen is flushed with a sterile saline solution to ensure all traces of infection have been removed.
ANCE00183

"Laparoscopic Placement of a
Peritoneal Dialysis Catheter"
Houston Methodist DeBakey Heart & Vascular Center, presents a cardiovascular procedure featuring Eric K. Peden, MD, Shri Timbalia, MD, and Kenneth Livingston as they demonstrate “Laparoscopic Placement of a
Peritoneal Dialysis Catheter".
Surgery: Eric K. Peden, MD, Shri Timbalia, MD, and Kenneth Livingston
Narration: Kenneth Livingston
** This medical education program may contain graphic content. **
_________________________________
A DeBakey CV Education event
Presented by Houston Methodist DeBakey Heart & Vascular Center.
Building on Dr. Michael E. DeBakey’s commitment to excellence in education, Houston Methodist DeBakey CV Education is an epicenter for cardiovascular academic and clinical educational programs that support the provision of optimal care to patients suffering from cardiovascular conditions and diseases.
FOR MORE INFORMATION
DeBakey CV Education:
https://www.houstonmethodist.o....rg/education/medical
For the latest education and training opportunities from DeBakey CV Education: http://bit.ly/HMdebakeyemail
Follow Us:
Facebook: https://www.facebook.com/debakeycvedu
Twitter: https://twitter.com/DeBakeyCVedu
Livestream: https://livestream.com/debakey
SmugMug: https://debakey.smugmug.com/
Want concise, relevant reviews of the hottest topics in CV medicine? Subscribe for FREE to the Methodist DeBakey Cardiovascular Journal for quarterly, peer-reviewed issues delivered to your door.
https://journal.houstonmethodist.org/

This surgical animation is for patient education and describes a laparoscopic colectomy, which is a type of minimally invasive surgery for colon cancer. Laparoscopic colectomy, also called minimally invasive colectomy, involves several small incisions in your abdomen. Instead of a big incision, the surgeon makes a few small cuts (0.5-1 centimeters) in the abdominal cavity to insert a surgical camera and instruments and perform the operation. A slightly bigger incision, about 3.5 centimeters wide, is made to remove the tumor.
When compared to traditional open surgery, laparoscopic colectomy can result in much less pain and swifter recovery. Depending on the procedure, most laparoscopic colectomy patients leave the hospital and return to normal activities more quickly than patients recovering from open surgery.
Colorectal cancer is the second leading cause of cancer death in the United States.
For more information about 3d animation videos, please visit https://www.amerra.com
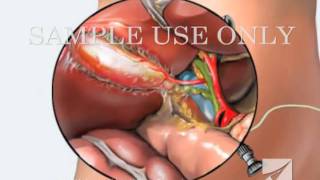
This medical animation shows laparoscopically assisted gallbladder removal surgery, or cholecystectomy. The animation begins by showing the normal anatomy of the liver and gallbladder. Over time, gallstones form within the gallbladder, blocking the cystic duct, and causing the gallbladder to become enlarged and inflamed. The procedure, sometimes called a "lap-chole", begins with the insertion of four trocar devices, which allow the physician to see inside the abdomen without making a large incision. Air is added to the abdominal cavity to make it easier to see the gall bladder. Next, we see a view through the laparascope, showing two surgical instruments grasping the gallbladder while a third severs the cystic duct. After the gallbladder is removed, the camera pans around to show that the cystic artery and vein, have already been clipped to prevent bleeding.
Item #ANIM026
