Seneste videoer
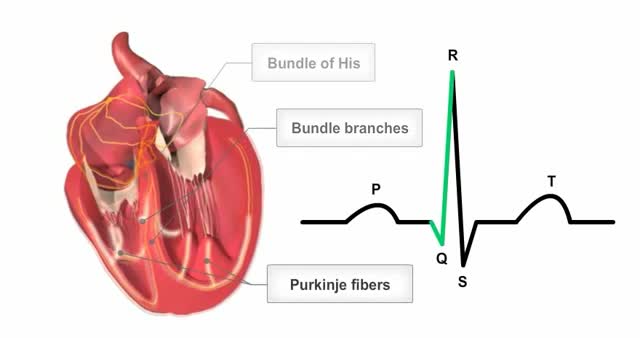
The heart's conductions system controls the generation and propagation of electric signals or action potentials causing the hearts muscles to contract and the heart to pump blood.

When you’re depressed, it can feel like you’ll never get out from under a dark shadow. However, even the most severe depression is treatable. So, if your depression is keeping you from living the life you want to, don’t hesitate to seek help. Learning about your depression treatment options will help you decide what approach is right for you. From therapy to medication to healthy lifestyle changes, there are many effective treatments that can help you overcome depression and reclaim your life.

Biliary atresia is a rare disease of the liver and bile ducts that occurs in infants. Symptoms of the disease appear or develop about two to eight weeks after birth. Cells within the liver produce liquid called bile. Bile helps to digest fat.

Gallbladder cancer is cancer that begins in the gallbladder. Your gallbladder is a small, pear-shaped organ on the right side of your abdomen, just beneath your liver. The gallbladder stores bile, a digestive fluid produced by your liver. Gallbladder cancer is uncommon. When gallbladder cancer is discovered at its earliest stages, the chance for a cure is very good. But most gallbladder cancers are discovered at a late stage, when the prognosis is often very poor. Gallbladder cancer is difficult to diagnose because it often causes no specific signs or symptoms. Also, the relatively hidden nature of the gallbladder makes it easier for gallbladder cancer to grow without being detected. Symptoms ShareTweet Aug. 07, 2014 References Products and Services Book: Mayo Clinic on Digestive Health Give today to find cancer cures for tomorrow See also Abdominal pain Can you recommend a diet after gallbladder removal? Chemo Targets Chemotherapy Chemotherapy and hair loss: What to expect during treatment Chemotherapy and sex: Is sexual activity OK during treatment? Chemotherapy nausea and vomiting: Prevention is best defense Show more Advertisement Mayo Clinic does not endorse companies or products. Advertising revenue supports our not-for-profit mission. Advertising & Sponsorship PolicyOpportunitiesAd Choices Mayo Clinic Store Check out these best-sellers and special offers on books and newsletters from Mayo Clinic. NEW! – The Mayo Clinic Diet, Second Edition Relief for America's epidemic of indigestion Keeping your bones healthy and strong Manage blood pressure for better health The Mayo Clinic Diet Online
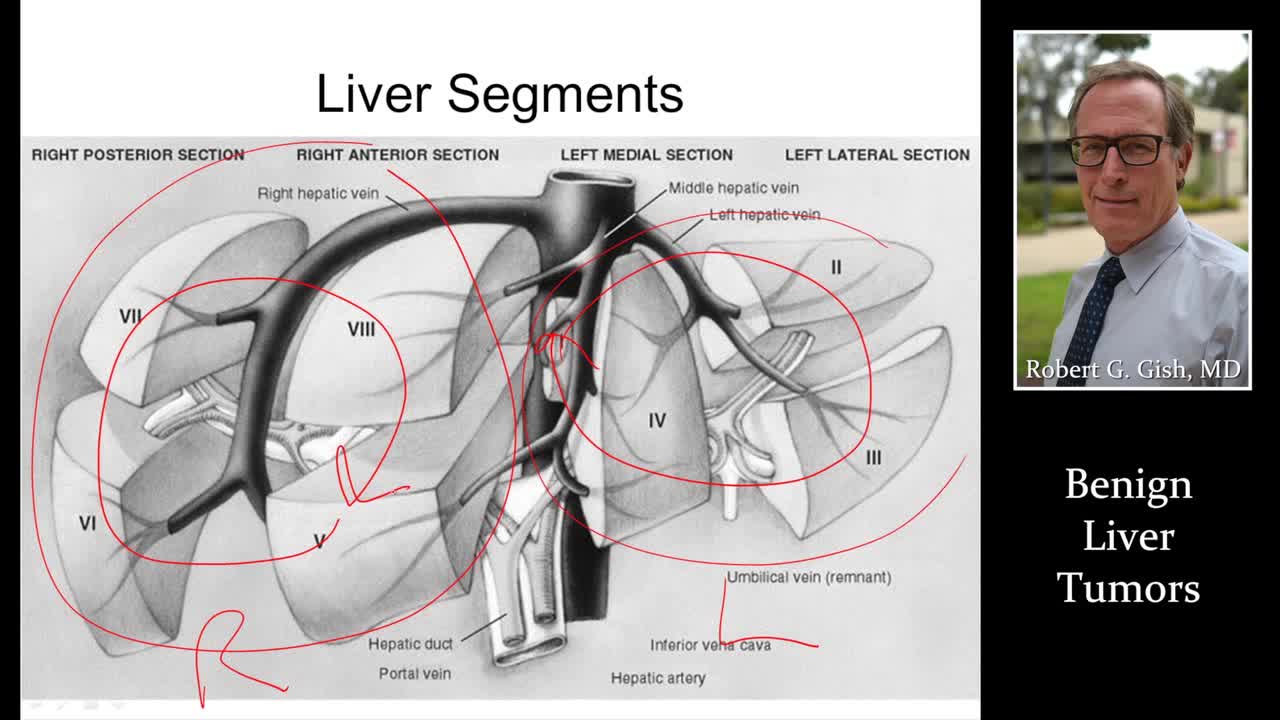
This form of liver cancer is called primary liver cancer. Noncancerous, or benign, liver tumors are common. They do not spread to other areas of the body, and they usually do not pose a serious health risk. In most cases, benign liver tumors are not detected because they cause no symptoms.
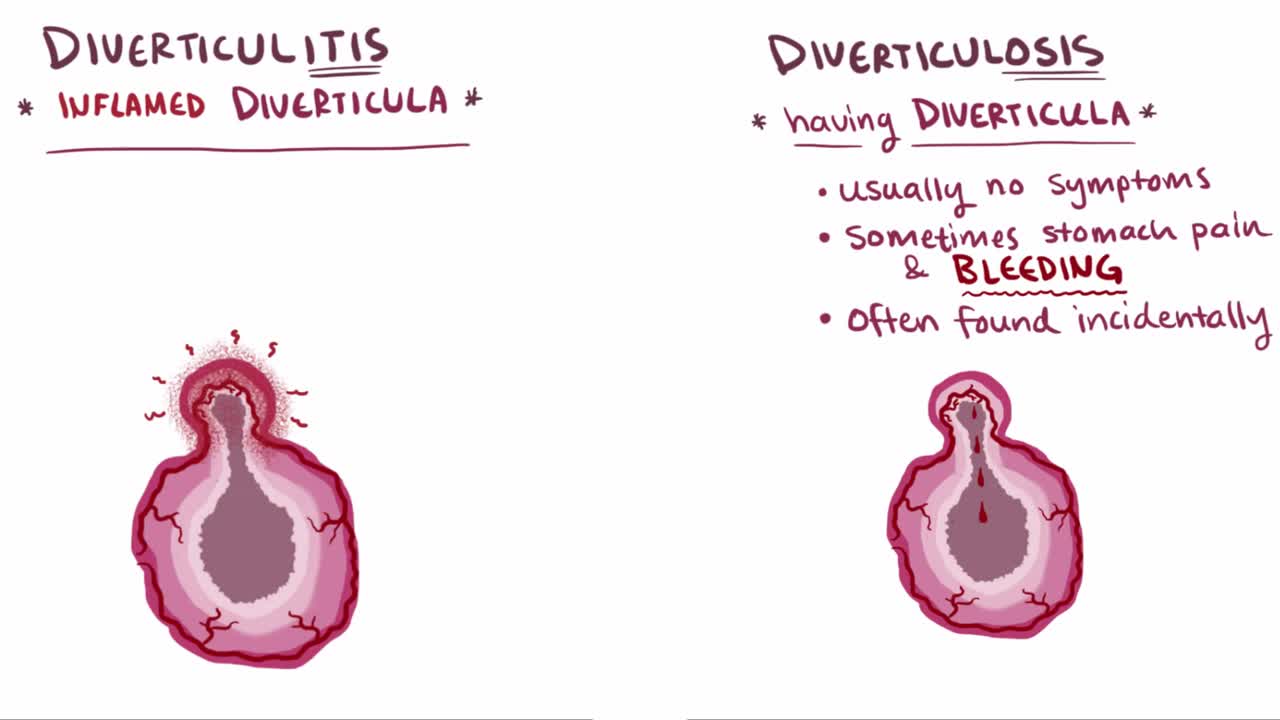
What are diverticula? Diverticula are outpouchings that most commonly happen in the sigmoid colon of the large intestine. The presence of a diverticulum is defined as diverticulosis, whereas diverticulitis describes an inflamed diverticulum

Hereditary hemochromatosis (he-moe-kroe-muh-TOE-sis) causes your body to absorb too much iron from the food you eat. Excess iron is stored in your organs, especially your liver, heart and pancreas. Too much iron can lead to life-threatening conditions, such as liver disease, heart problems and diabetes.
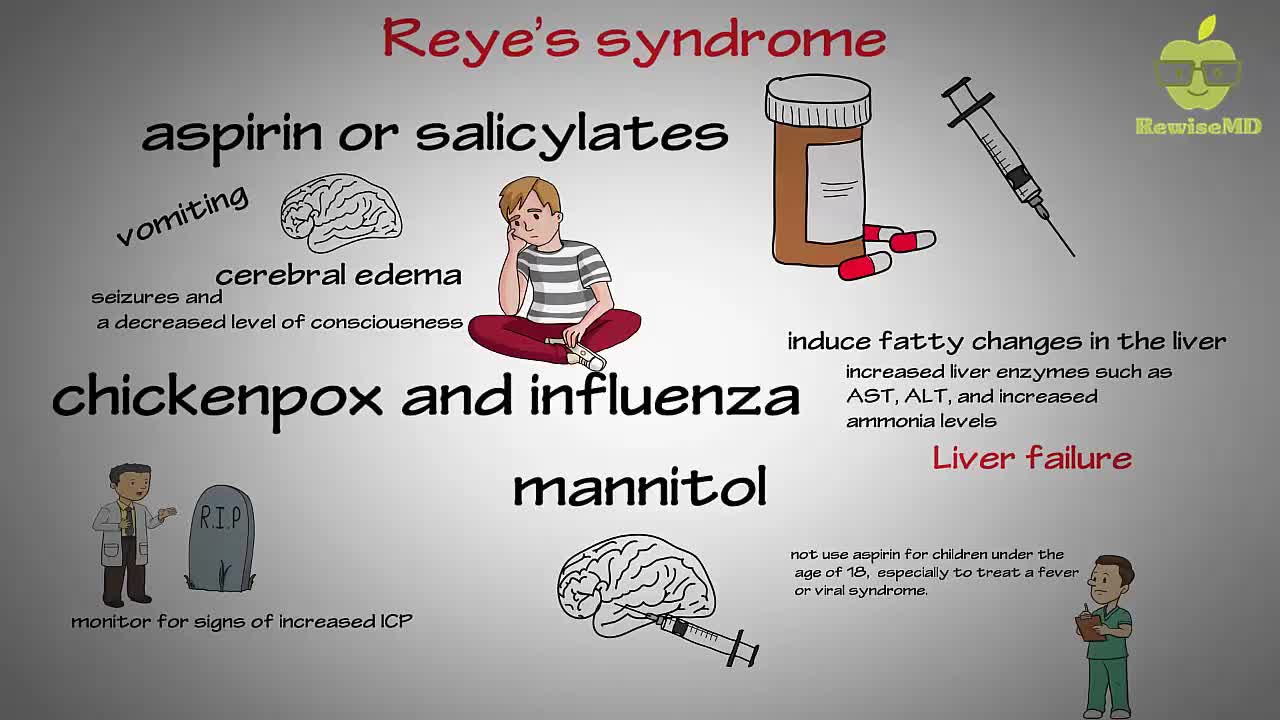
In Reye's syndrome, a child's blood sugar level typically drops while the levels of ammonia and acidity in his or her blood rise. At the same time, the liver may swell and develop fatty deposits. Swelling may also occur in the brain, which can cause seizures, convulsions or loss of consciousness. The signs and symptoms of Reye's syndrome typically appear about three to five days after the onset of a viral infection, such as the flu (influenza) or chickenpox, or an upper respiratory infection, such as a cold
People with lactose intolerance are unable to fully digest the sugar (lactose) in milk. As a result, they have diarrhea, gas and bloating after eating or drinking dairy products. The condition, which is also called lactose malabsorption, is usually harmless, but its symptoms can be uncomfortable. A deficiency of lactase — an enzyme produced in your small intestine — is usually responsible for lactose intolerance. Many people have low levels of lactase but are able to digest milk products without problems. If you're actually lactose intolerant, though, your lactase deficiency leads to symptoms after you eat dairy foods.
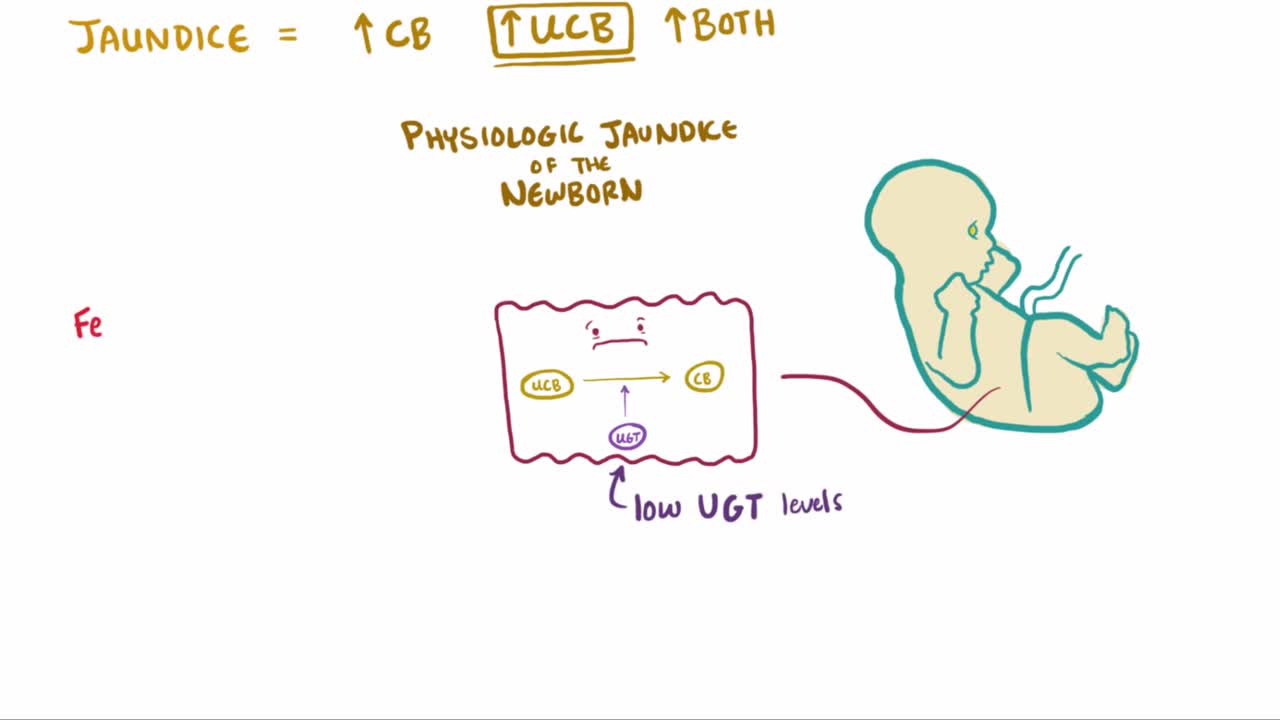
What is jaundice? Well, jaundice is a condition where the skin and eyes take on a yellowish color due to increased levels of bilirubin in the bloodstream

Biliary Colic Examination
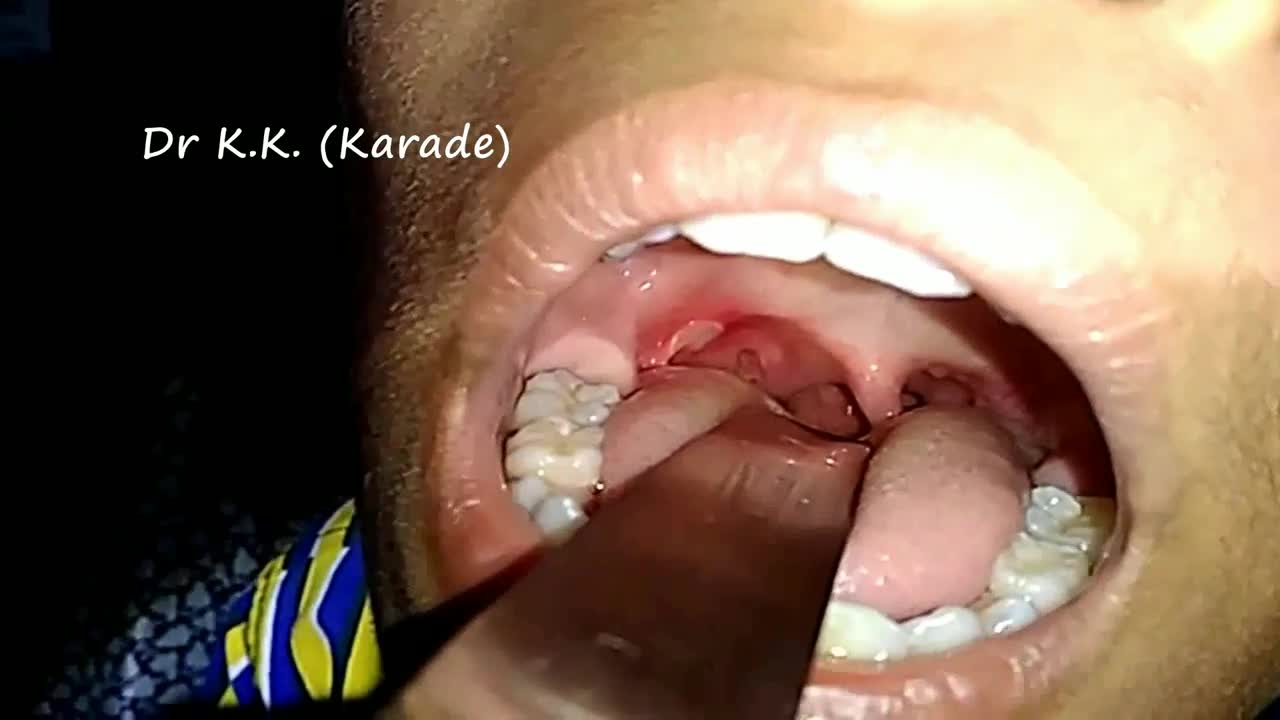
Canker sores (Aphthous ulcer) are small, painful ulcers on the inside of the mouth, tongue, lips, or throat.Canker sores are white or yellow and surrounded by a bright red area. They are not cancerous.
Behcet's (beh-CHETS) disease, also called Behcet's syndrome, is a rare disorder that causes blood vessel inflammation throughout your body. The disease can lead to numerous signs and symptoms that may seem unrelated at first. They may include mouth sores, eye inflammation, skin rashes and lesions, and genital sores. The effects of Behcet's disease vary from person to person and may clear up on their own. Treatment involves medications to reduce the signs and symptoms of Behcet's disease and to prevent serious complications, such as blindness.

Sialadenitis is an infection of the salivary glands. It is usually caused by a virus or bacteria . The parotid (in front of the ear) and submandibular (under the chin) glands are most commonly affected. Sialadenitis may be associated with pain, tenderness, redness, and gradual, localized swelling of the affected area.
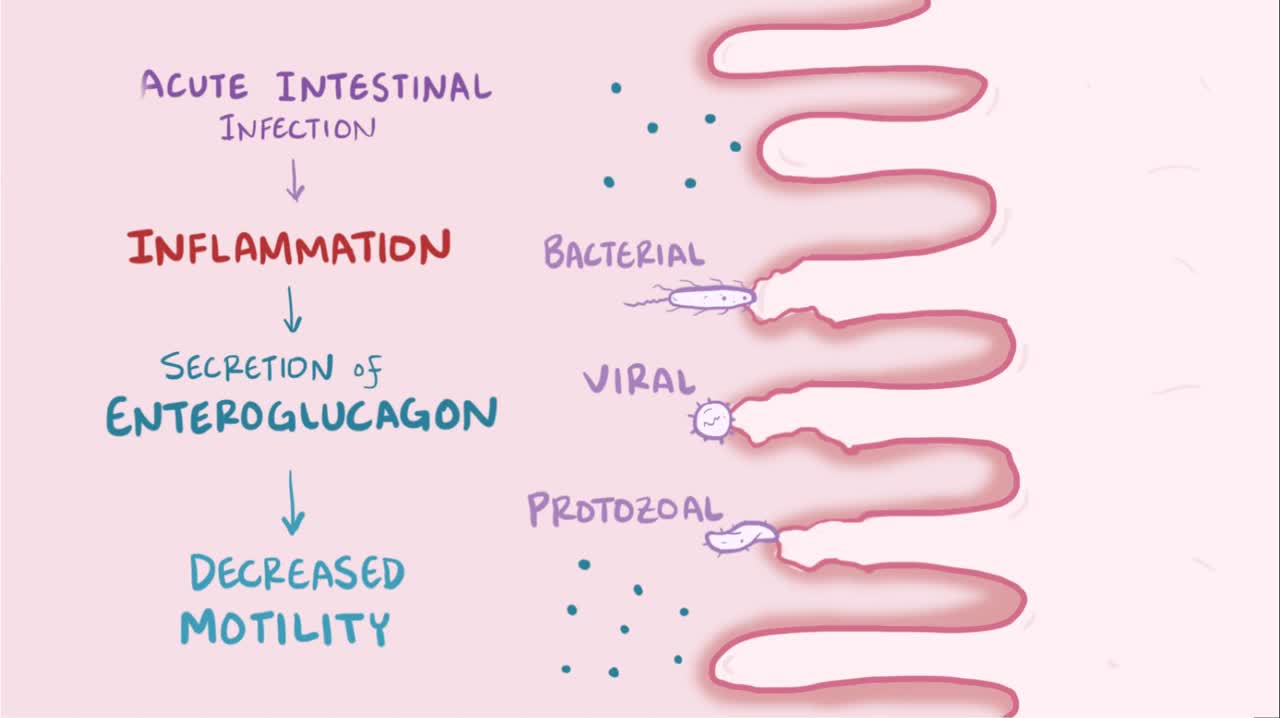
What is tropical sprue? Tropical sprue is diagnosed when somebody has long-standing GI problems and has visited tropical regions in the past. It's thought to be caused by bacterial overgrowth and often leads to villous atrophy.

HSV-1 causes "cold sores" on the mouth, and up to 80% of the population has this virus. However, HSV-1 may also be transmitted to the genitals through oral/genital sex and about 40% of genital herpes is caused by HSV-1. Up to 22% of sexually active adults have genital herpes caused by HSV-2.
Duodenal atresia, also known as duodenojejunal atresia, is the congenital absence or complete closure of a portion of the lumen of the duodenum. It causes increased levels of amniotic fluid during pregnancy (polyhydramnios) and intestinal obstruction in newborn babies.
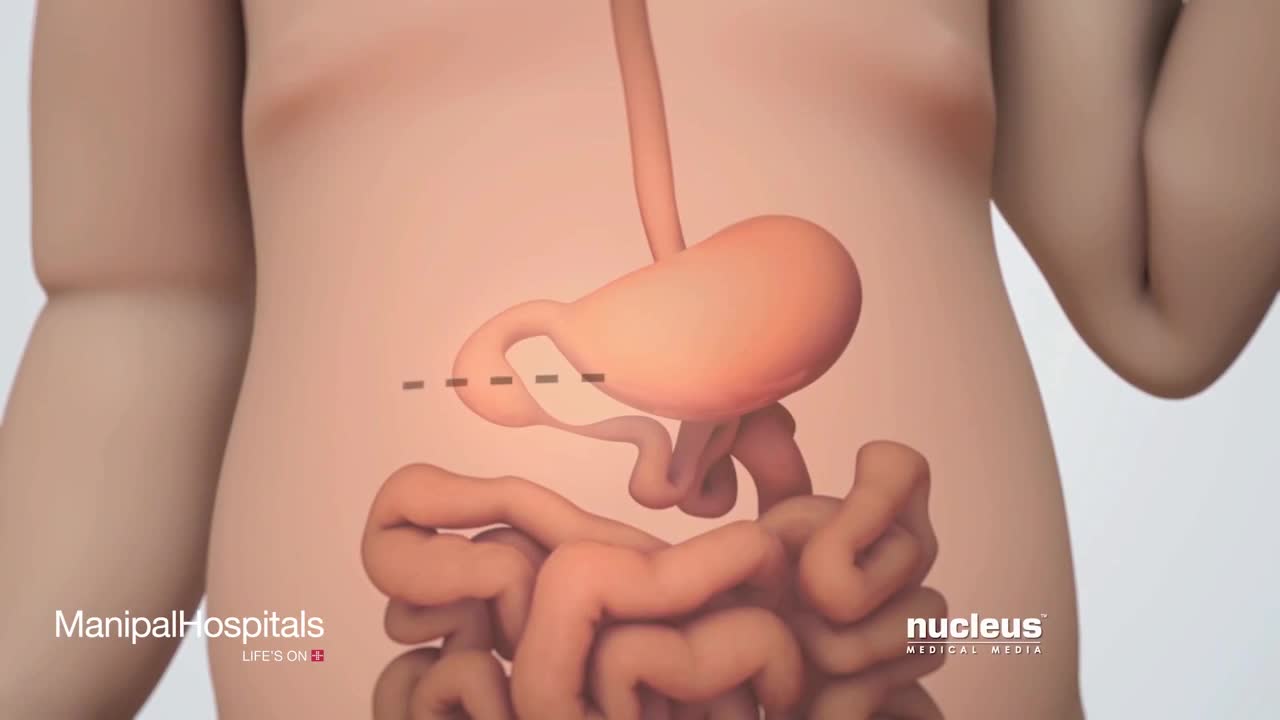
Hypertrophic pyloric stenosis (HPS) causes a functional gastric outlet obstruction as a result of hypertrophy and hyperplasia of the muscular layers of the pylorus. In infants, HPS is the most common cause of gastric outlet obstruction and the most common surgical cause of vomiting.
The gastrointestinal tract (GIT) arises initially during the process of gastrulation from the endoderm of the trilaminar embryo (week 3) and extends from the buccopharyngeal membrane to the cloacal membrane. The tract and associated organs later have contributions from all the germ cell layers. During the 4th week three distinct regions (fore-, mid- and hind-gut) extend the length of the embryo and will contribute different components of the GIT. The large mid-gut is generated by lateral embryonic folding which "pinches off" a pocket of the yolk sac, the 2 compartments continue to communicate through the vitelline duct. The oral cavity (mouth) is formed following breakdown of the buccopharyngeal membrane (oropharyngeal or oral membrane) and contributed to mainly by the pharynx lying within the pharyngeal arches (More? Head Development). Loss of buccopharyngeal membrane opens the tract to amniotic fluid through the remainder of development, and during the fetal period is actively swallowed.

Gastroschisis is a birth defect that develops in a baby while a woman is pregnant. This condition occurs when an opening forms in the baby's abdominal wall. The baby's bowel pushes through this hole. It then develops outside of the baby's body in the amniotic fluid.
