Neueste Videos

a video showing fiberoptic laryngoscopy and bronchoscopy

4D Ultrasound 23 Weeks
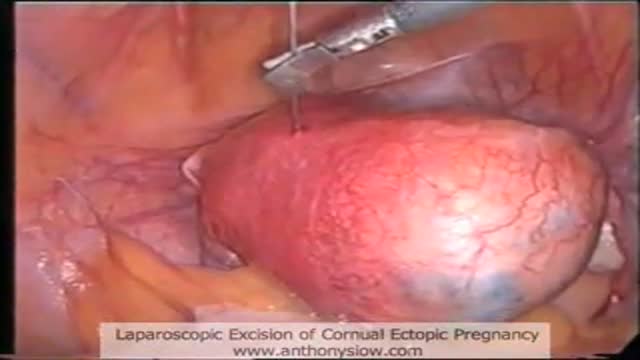
Laparoscopic excision of a 6cm Cornual Ectopic Pregnancy that failed initial MTX treatment.

Removal of pregnancy within the fallopain tube using laparoscopic keyhole surgery. A segment of the tube together with the pregnancy within is removed.

A video showing the Vasa Previa which is an abnormality of the placenta

A video showing Cystocele Repair
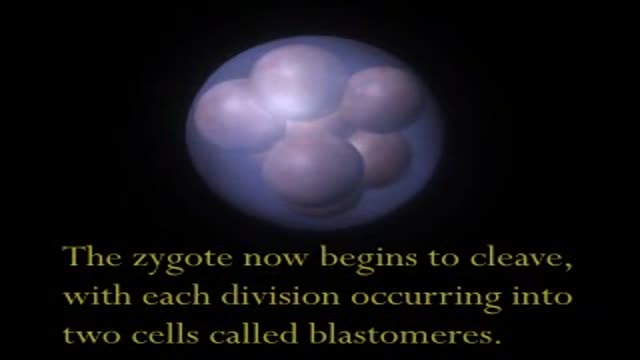
This video shows the process of development and growth of the fetus intrauterine.

Male Urethral Prostate Stent/Catheter.Removal and insertion.

How to apply a splint on a broken bone

Rest
Ice
Compression
Elevation

Physical Exam and Sample History

An Emergency Medicine video showing how to perform Jaw Thrust technique

Initial Assessment

How to deal with a case of ingested poison

Infant Cardio-pulmonary Resuscitation

Infant Airway Obstruction and how to deal with

A video showing impaled objects

How to deal with heart attack and with stroke

how to to deal with fractures and dislocations
How to move a patient during an accident or during emergency
