- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Latest videos

Symptoms of depression in women include: Persistent sad, anxious, or "empty" mood. Loss of interest or pleasure in activities, including sex. Restlessness, irritability, or excessive crying. Feelings of guilt, worthlessness, helplessness, hopelessness, pessimism. Sleeping too much or too little, early-morning awakening.

Everyone feels sad or low sometimes, but these feelings usually pass with a little time. Depression—also called “clinical depression” or a “depressive disorder”—is a mood disorder that causes distressing symptoms that affect how you feel, think, and handle daily activities, such as sleeping, eating, or working. To be diagnosed with depression, symptoms must be present most of the day, nearly every day for at least 2 weeks.

Nearly 300 million people experience the world without certain colors every day. ‘Color For the Colorblind’ is a short documentary about what happened when we partnered with EnChroma, maker of color blindness-correcting glasses, to help people experience colors for the first time.

Huge CYST in Abdomin

Usually a sebaceous cyst grows very slowly and doesn't cause pain. However, they can become inflamed or infected, with the overlying skin becoming red, tender, and sore. Sometimes, they occur on a site that is constantly irritated, such as a cyst on your neck that rubs against your collar.

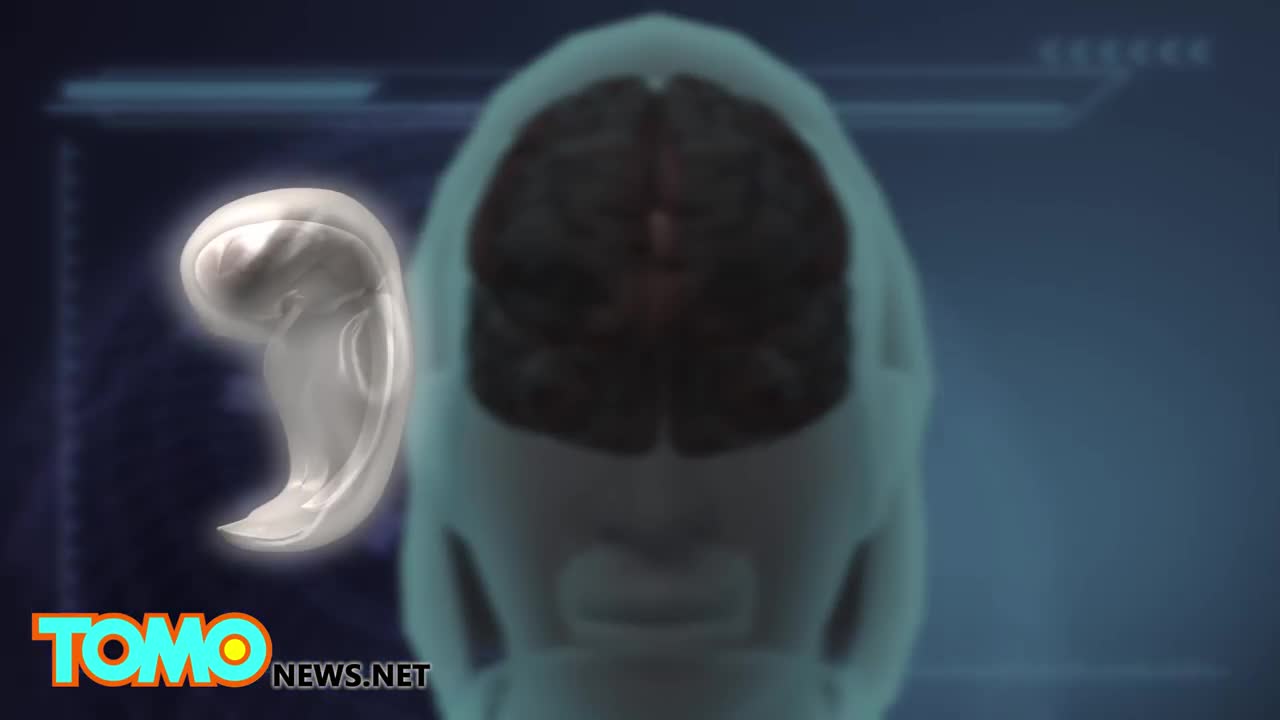
People whose back or neck pain has not been relieved by back surgery or other treatments may have another option to consider: spinal cord stimulation. Around the world, some 14,000 patients undergo spinal cord stimulator implants each year. Spinal cord stimulation (SCS) delivers mild electrical stimulation to nerves along the spinal column, modifying or blocking nerve activity in a non-medicinal way to minimize the sensation of pain reaching the brain.

Our nervous system is involved in everything our body does, from maintaining our breath to controlling our muscles. Our nerves are vital to all we do; therefore, nerve pain and damage can heavily influence our quality of life. In Discovery News' latest video, "Why Can't We Reverse Nerve Damage?" host Lissette Padilla explains the central nervous system (CNS) has certain proteins that inhibit cell regeneration, because each cell in the nervous system has a unique function on the pathway, like a circuit, and can't be replaced.
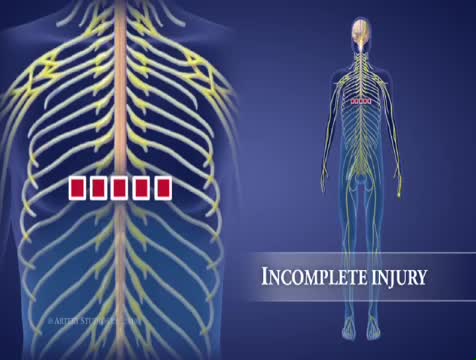
High-Cervical Nerves (C1 – C4) Most severe of the spinal cord injury levels Paralysis in arms, hands, trunk and legs Patient may not be able to breathe on his or her own, cough, or control bowel or bladder movements. Ability to speak is sometimes impaired or reduced. When all four limbs are affected, this is called tetraplegia or quadriplegia. Requires complete assistance with activities of daily living, such as eating, dressing, bathing, and getting in or out of bed May be able to use powered wheelchairs with special controls to move around on their own Will not be able to drive a car on their own Requires 24-hour-a-day personal care
U.S. biotech firm Bioquark recently got approval to move forward with its ReAnima Project, in which it will try to reverse brain death in patients on life support

Researchers have received approval to bring 20 brain-dead humans back to life.
Very small currents can be imperceptible. Larger current passing through the body may make it impossible for a shock victim to let go of an energized object. Still larger currents can cause fibrillation of the heart and damage to tissues. Death caused by an electric shock is called electrocution.
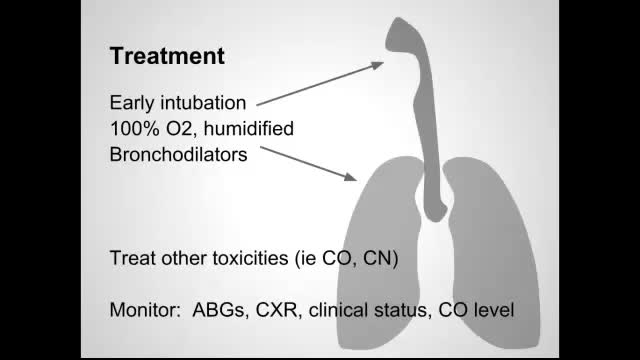
Smoke inhalation is the leading cause of death due to fires. It produces injury through several mechanisms, including thermal injury to the upper airway, irritation or chemical injury to the airways from soot, asphyxiation, and toxicity from carbon monoxide (CO) and other gases such as cyanide.

Giant cell tumour is a locally aggressive primary bone tumour, located eccentrically in the metaphysis and epiphysis of a long bone. It commonly affects distal end of Femur, proximal end of Tibia and distal end of Radius. It is occasionally reported in small bones of hand and foot[1], spine[2] and pelvis[3]. Though it occurs in 20 - 35 year old individuals commonly, it can also be seen in children as young as 2 years[4] and also in older individuals
Parasitic twins: boy carrying dead twin inside him, giant tumor removed - tumors compilation
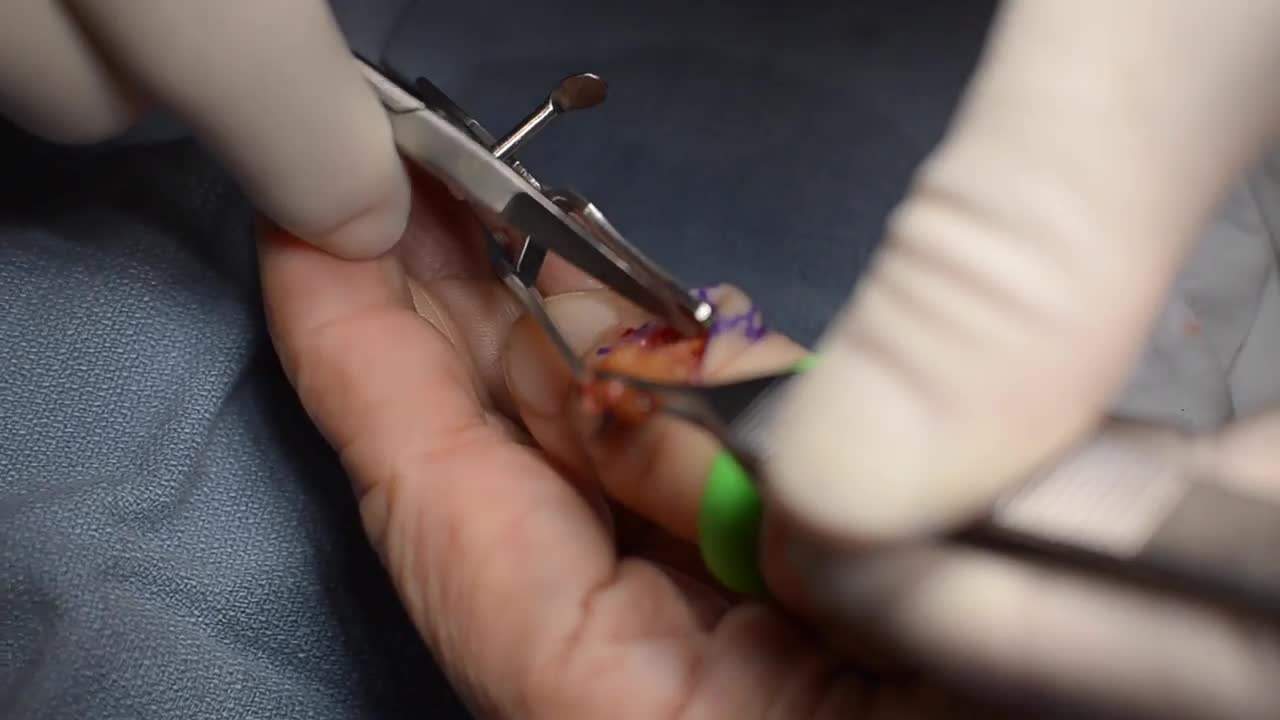
GIANT CELL TUMOR REMOVAL Plastic, Cosmetic and Reconstructive
Despite the effective diagnostic and treatment options available today, Dr. Wolfe notes that he continues to see a high number of untreated scaphoid fractures that have progressed to nonunion. However, he adds that this may not be the result of a missed diagnosis, but rather more related to the relatively innocuous injury that causes a low level of suspicion. Recognition and awareness of scaphoid fractures is higher today among primary care providers, emergency room physicians, pediatricians, and sports trainers, but fully 15% of patients with suggestive physical findings and normal initial x-rays will have an “occult”, or concealed, scaphoid fracture. Specialized imaging studies are critical at an early stage to reduce the chance of scaphoid nonunion.
A blood test to measure calcium, phosphorous and vitamin D levels can usually confirm a diagnosis of rickets, although your child may also have some X-rays or possibly a bone density scan (DEXA scan). This is a type of X-ray that measures the calcium content in bones.

Down syndrome is a set of physical and mental traits caused by a gene problem that happens before birth. Children who have Down syndrome tend to have certain features, such as a flat face and a short neck. They also have some degree of intellectual disability. This varies from person to person. But in most cases it is mild to moderate.

Down’s Syndrome Twins Are One In A Million
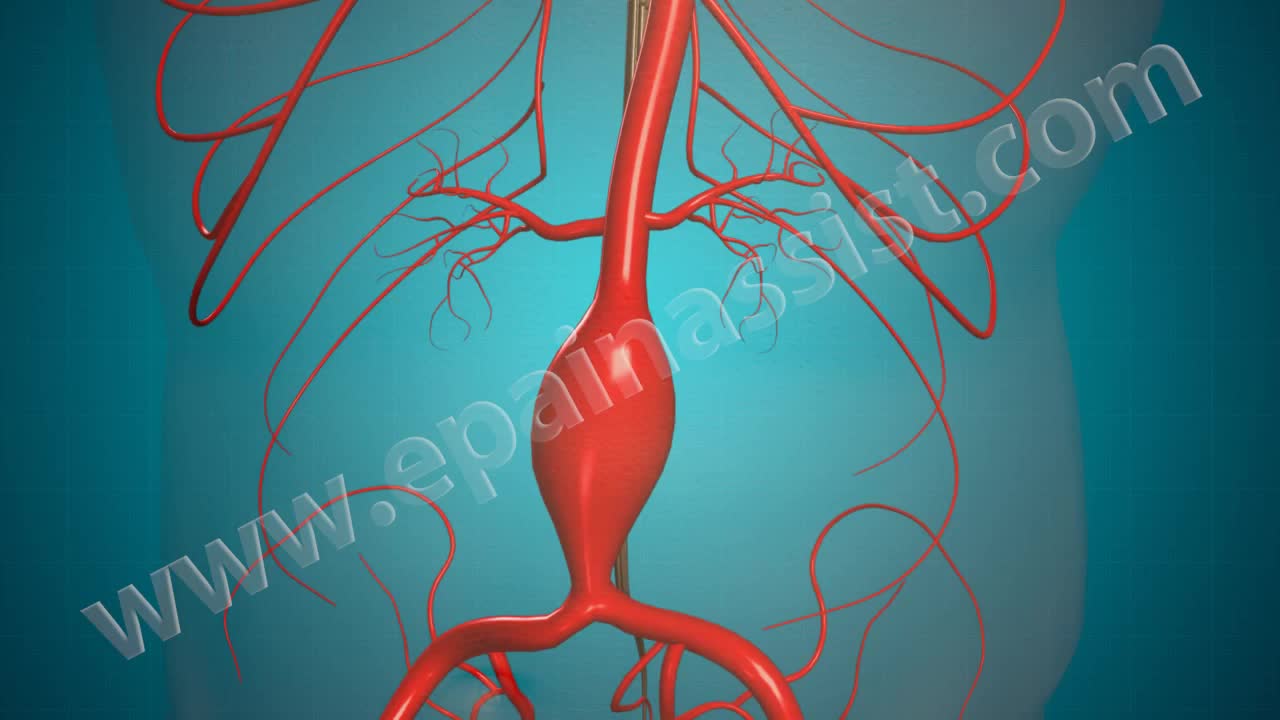
Open Abdominal Aortic and Endovascular Aneurysm Repair Surgery
