- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
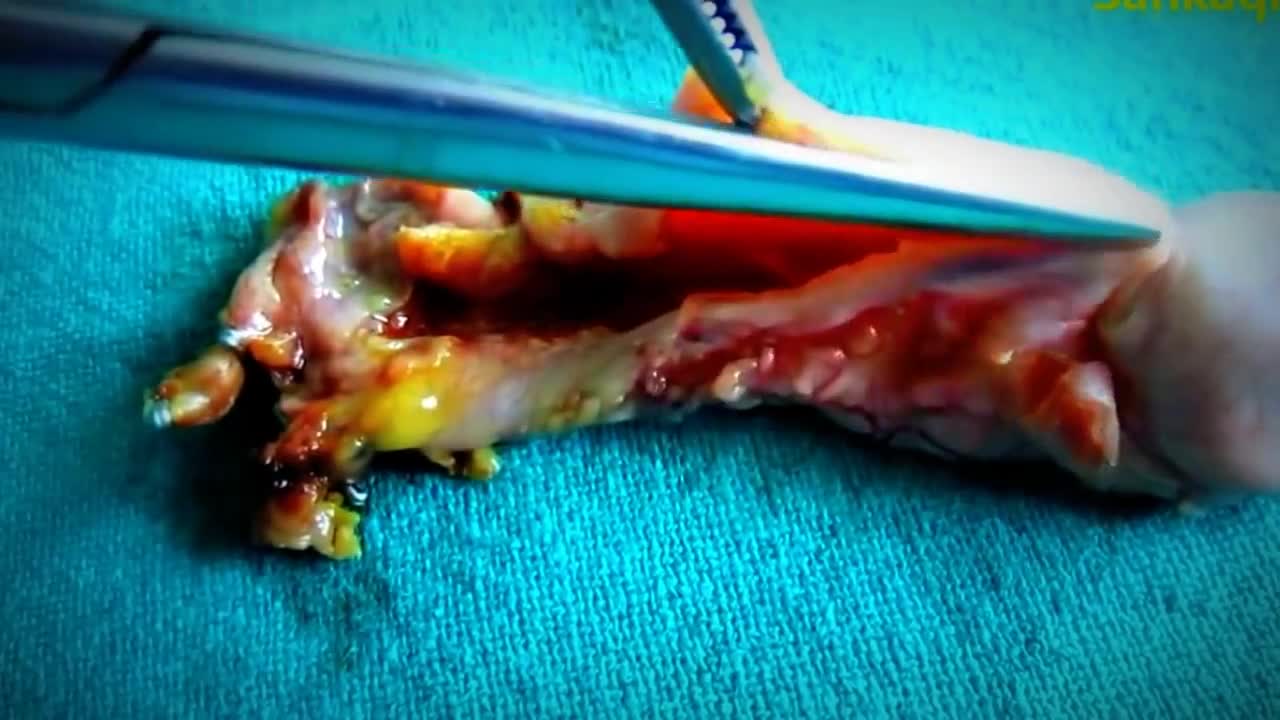
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Latest videos

Is There A Way To Know If I Have An Aortic Aneurysm Before It Ruptures?
Your body needs bile, but if it has too much cholesterol in it, that makes gallstones more likely. It can also happen if your gallbladder can't empty properly. Pigment stones are more common in people with certain medical conditions, such as cirrhosis (a liver disease) or blood diseases such as sickle cell anemia.
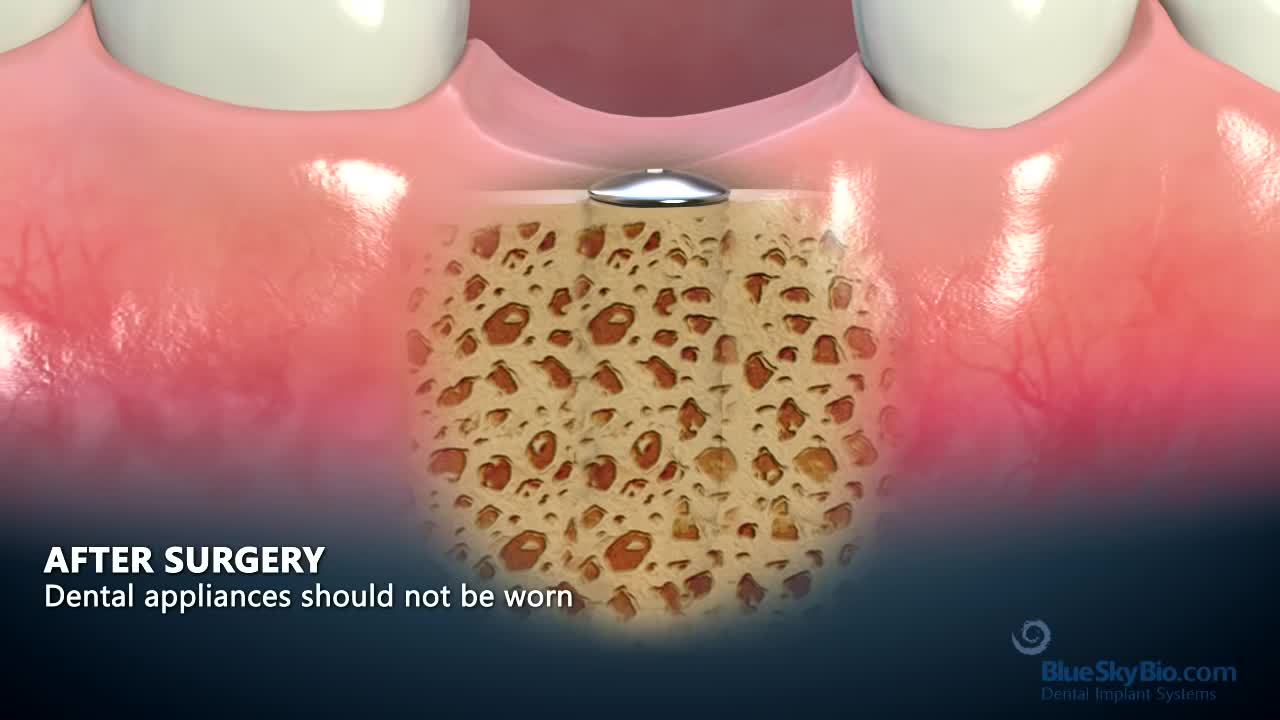
The dental implant, usually a cylindrical and/or tapered post made of titanium, is placed surgically into the jawbone. As you heal, your implant will osseointegrate, or fuse with, your natural jawbone, with the two growing together to form a strong and long-lasting foundation for your replacement teeth.
Tooth loss can make you look older. When you lose a tooth and don’t replace it with a dental implant, you risk the chance of jawbone loss. Normally, your tooth root stimulates the continued growth and health of your jawbone. Dental implants mirror your natural tooth root and keep your jawbone healthy.

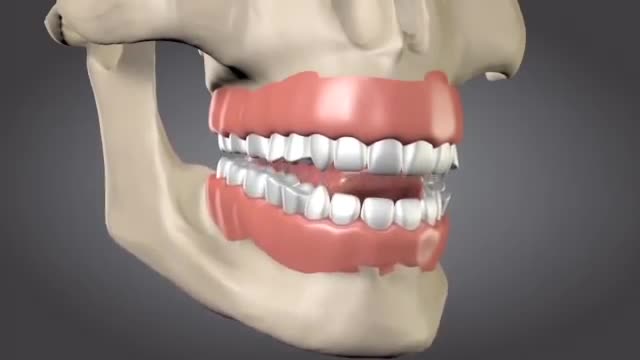
Aim: To detail two different clinical protocols and case studies using mini-implant anchorage developed to respond to certain clinical conditions. Methods: Two clinical protocols are described to upright mesially tilted mandibular molars. In the first protocol, a single mini-implant is inserted distally to the molar to be uprighted, and an elastic traction chain is applied to the tooth. In the second clinical approach, two mini-implants are inserted mesially. A screw-suspended TMA sectional archwire is applied (Derton-Perini technique). Two cases, descriptive of the two different treatment protocols, are described. In the first case, the mandibular right second premolar was missing and the adjacent first molar needed to be uprighted. A single screw was inserted distally to the first molar, and an elastic chain was applied. In the second case, the mandibular left second molar was missing and the third molar needed to be uprighted. Two mini-implants were inserted mesially and a fully screw-supported sectional archwire was used to upright and bodily mesialize the third molar. Results: Both uprighting approaches uprighted the molar axis without loss of anchorage. Conclusion: The two approaches to mandibular molar uprighting, developed as rational responses to different clinical cases, were both found to be effective. Research paper: Mandibular molar uprighting using mini-implants: Different approaches for different clinical cases-Two case reports.. Available from: https://www.researchgate.net/publication/224920305_Mandibular_molar_uprighting_using_mini-implants_Different_approaches_for_different_clinical_cases-Two_case_reports [accessed
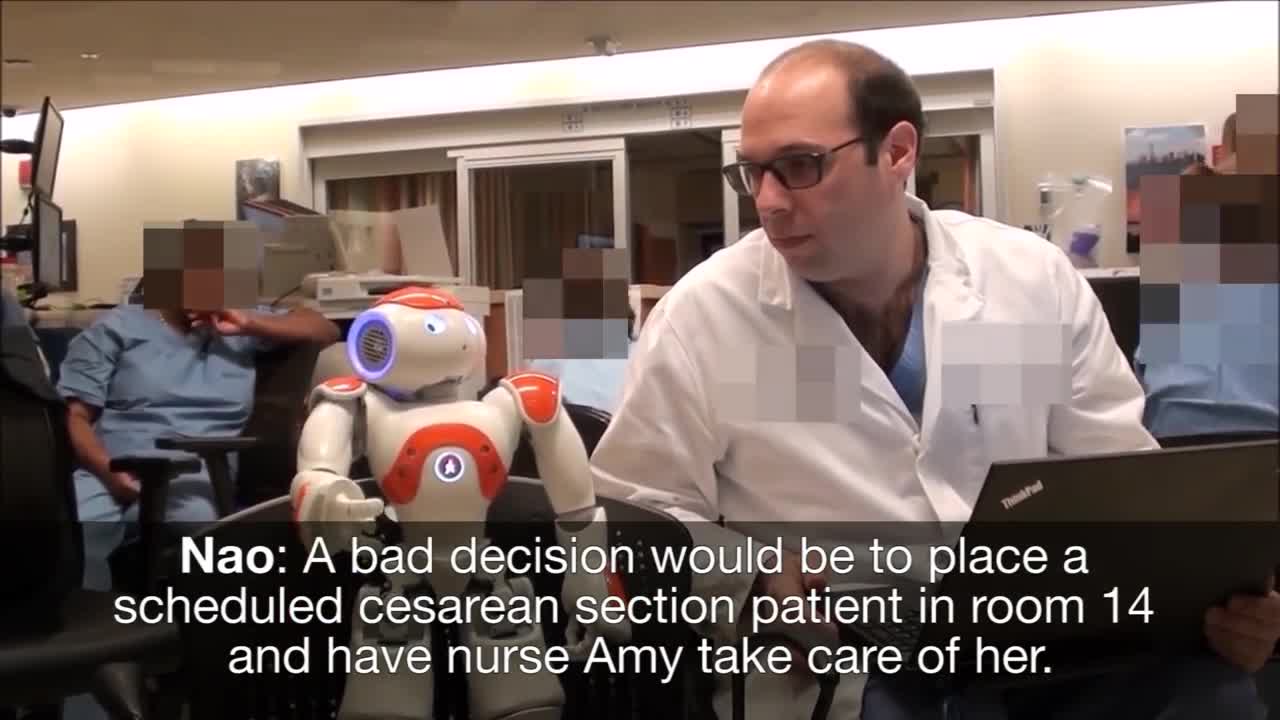
Medical Robot Assistants, new technology

SPIDER Surgery-- Single Incision Gallbladder Removal

The primary goal of treatment for each patient is to help relieve pain and other symptoms resulting from the herniated disc. To achieve this goal, each patient’s treatment plan should be individualized based on the source of the pain, the severity of pain and the specific symptoms that the patient exhibits.
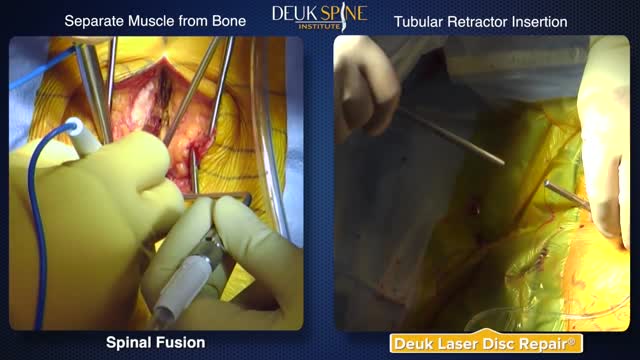
Deuk Laser Disc Repair vs Traditional Spinal Fusion Comparison, Laser versus Fusion
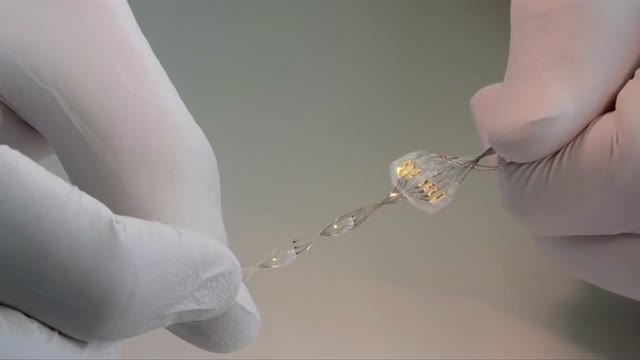
Scientists in Switzerland proved in 2012 that electrical-chemical stimulation of the spinal cord could restore lower body movement in paralysed rats.

Instead of permanently joining (fusing) vertebrae with metal rods and screws, and therefore restricting movement, the new procedure uses the Anatomic Facet Replacement System (AFRS) device that attaches to each of two adjacent vertebrae with a movable joint that mimics the spine's natural joint.

Removal of a Broken Intramedullary Nail and Exchange Nailing for Tibial Nonunion

This video shows the technique of suprapatellar tibial nailing as used for a segmental tibia fracture. The broken leg was treated with the nail to allow immediate mobility and range of motion; no cast was needed for this injury.

A ganglion cyst is a tumor or swelling on top of a joint or the covering of a tendon (tissue that connects muscle to bone). It looks like a sac of liquid (cyst). Inside the cyst is a thick, sticky, clear, colorless, jellylike material. Depending on the size, cysts may feel firm or spongy.

A nonsurgical method of treating a ganglion is to drain the fluid from (aspirate) the ganglion sac. Your doctor can do this in the office using the following procedure: The ganglion area is cleaned with an antiseptic solution. A local anesthetic is injected into the ganglion area to numb the area. When the area is numb, the ganglion sac is punctured with a sterile needle. The fluid is drawn out of the ganglion sac. The ganglion collapses. A bandage and, in some cases, a splint are used for a few days to limit movement and prevent the ganglion sac from filling again. Treating a ganglion by draining the fluid with a needle may not work because the ganglion sac remains intact and can fill again, causing the ganglion to return. For this reason, your doctor may puncture the sac with the needle 3 or 4 times so the sac will collapse completely. Even then, the ganglion is likely to come back.
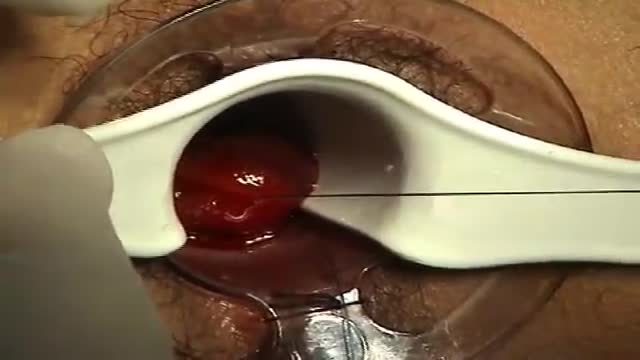
minimally invasive procedure is the new gold standard for hemorrhoidectomy, according to American and European experts in the field. The procedure, known as PPH (procedure for prolapse and hemorrhoids) stapled hemorrhoidectomy, combines hemorrhoidal devascularization and repositioning to return the veins to the anal canal. “This year, this is the revolutionary new procedure in the United States,” Gary Hoffman, MD, clinical faculty member in general and colorectal surgery, Cedars-Sinai Medical Center, Los Angeles, told General Surgery News after moderating a live PPH telesurgery at the 2003 annual meeting of the Society of American Gastrointestinal Endoscopic Surgeons.
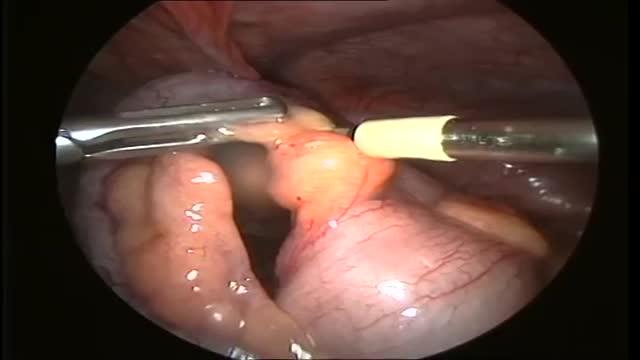
One thing we do know: We can live without it, without apparent consequences. Appendicitis is a medical emergency that requires prompt surgery to remove the appendix. Left untreated, an inflamed appendix will eventually burst, or perforate, spilling infectious materials into the abdominal cavity.

The first operation is harvesting the heart from the donor. The donor is usually an unfortunate person who has suffered irreversible brain injury, called "brain death". Very often these are patients who have had major trauma to the head, for example, in an automobile accident. The victim's organs, other than the brain, are working well with the help of medications and other "life support" that may include a respirator or other devices. A team of physicians, nurses, and technicians goes to the hospital of the donor to remove donated organs once brain death of the donor has been determined. The removed organs are transported on ice to keep them alive until they can be implanted. For the heart, this is optimally less than six hours. So, the organs are often flown by airplane or helicopter to the recipient's hospital.
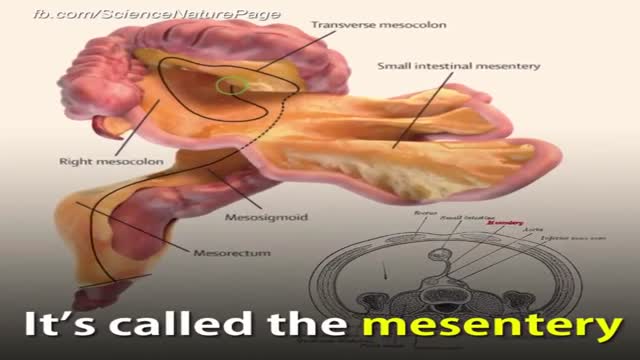
There is a new organ in your digestive system SHOW MORE

A Chinese hospital in the process of creating a human ear almost entirely through the human anatomy alone.
