- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Latest videos
Examination of lumbar spines

Examination of the hand and the wrist
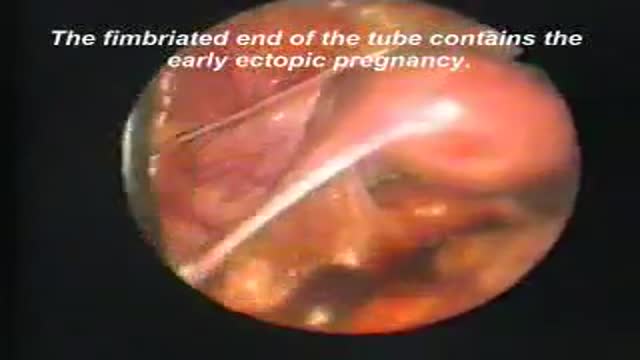
Laparoscopic removal of ectopic pregnancy

full examination of the foot and ankle

Examination of the cervical spines

Examination of peripheral pulses of the lower limb

Complete examination of the abdomen including all the items: inspection, palpation, percussion and auscultation Video

Examination of the heart and lungs with heart sounds

Observation of both jugular veins can provide a reliable indication of the volume and pressure in the right side of the heart since internal jugular veins pulsate in response to phasic changes in right atrial pressure. Proper positioning of the patient to increase the effects of gravity enhances distention of the jugular veins and, therefore, increases the ability to observe venous pulsations.

the most funny medical examination ever..Not: do not try at your office or clinic

Full complete clinical examination of the chest, lungs and respiration with breath sounds

Complete examination of the back

Complete clinical assessment and examination of the neck

Clinical complete examination of the mouth and throat

Complete clinical examination of the ears with all the associated tests

Examination of the eye,vision,retina and field of vision

It is very important to instruct your patients about how to self exam their breasts for any abnormalities or masses for early detection of any changes

Examination of the lymph nodes of the head

Optimal blood pressure typically is defined as 120 mm Hg systolic — which is the pressure as your heart beats — over 80 mm Hg diastolic — which is the pressure as your heart relaxes. For your resting heart rate, the target is between 60 and 100 beats per minute (bpm)

Breast masses are broadly classified as benign or malignant. Common causes of a benign breast mass include fibrocystic disease, fibroadenoma (see the image below), intraductal papilloma, and abscess.
