- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

DMC Pediatric Plastic and Reconstructive Surgeon Dr Arlene Rozzelle and her team of specialists repair a newborn’s cleft lip.

Have you ever swallowed something that wasn`t meant to be ingested?

One of the various variations of trabeculectomy...

Circumcision by Dissection method

A video showing the circumcision of a male baby

How to memorize more in pharma: Drug names, dental implications, numbers

How to give Intramuscular (IM) injection

Gastrointestinal GI Drug Delivery
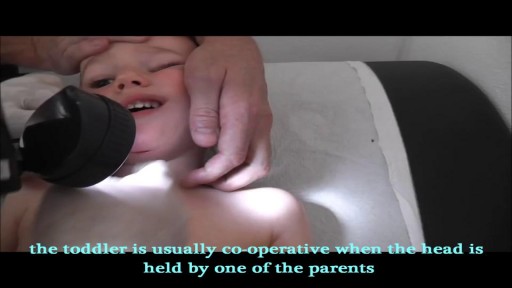
Human Glue used to repair a cut in the chin of a toddler
How to deal with chemical burns and their first aid
Minor burns can typically be treated at home -- but it's important to know when you need to seek treatment.

Vetical Mattress Suture

Watch that Baby Abortion Medical Procedure

Skin isn't just your body's biggest organ-- it's also the fastest growing.
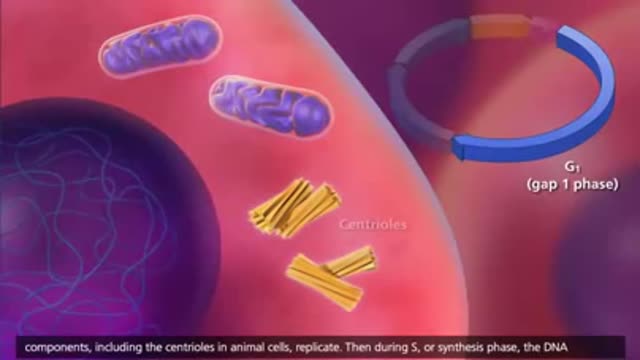
The cell cycle or cell-division cycle is the series of events that take place in a cell leading to its division and duplication of its DNA (DNA replication) to produce two daughter cells.


Heart sounds S1, S2

Dr. Daniel Del Vecchio, Harvard trained plastic surgeon, performs his breast lift technique, filling the upper portion of the breast for added volume
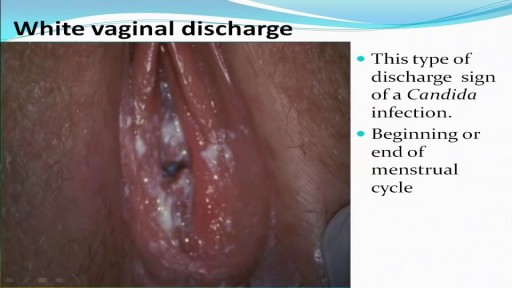
All you need to know about the Types of Female Genital Discharge
