- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Routine pelvic exams are important for good reproductive health. A woman should have her first GYN exam when she first thinks about becoming sexually active, when she becomes sexually active or when she turns 18.
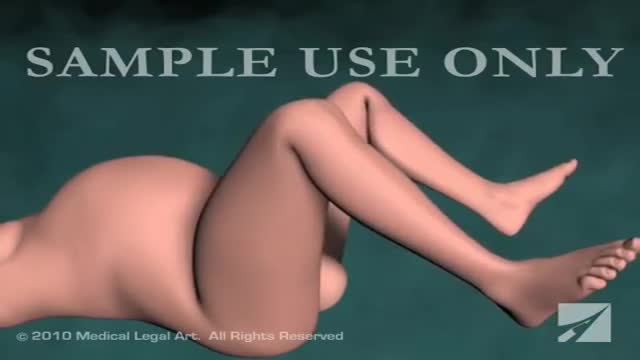
At the gynecologist, you will have a short general physical exam, including a breast exam. You will wear a hospital gown and nothing else. For the actual pelvic examination, you will lie down on an examination table with your feet resting in elevated “stirrups” (props that support your legs in the air). Stirrups might look a little scary, but they are there to keep you comfortable. Your legs will be spread apart, with your knees falling to each side so that your vagina is exposed. You may feel uncomfortable, but relax and realize that everyone goes through this.
External Exam
The practitioner will visually examine your vulva for discoloration, irritation, swelling and other abnormalities, and will gently feel for glands.
Internal Exam
There are two parts to the internal exam. The first involves a speculum, a metal or plastic instrument that the practitioner inserts into the vagina. The speculum is shaped like a duck’s bill, and once it is inserted into the vaginal canal, it is gently widened to spread the interior vaginal walls (this is not painful). As the vaginal walls are spread, the practitioner is able to see the walls of the vagina itself, and up the vaginal canal to the cervix. When viewing the vaginal canal and the cervix, the practitioner can look for discoloration, abnormal discharge, lesions, growths and signs of infection. It is possible for you to look at your own cervix during this process by propping yourself up on your elbows and using a mirror. Some practitioners ask if you would like to do this, but feel free to ask to if she doesn’t mention it first.
Pap Smear
Next the practitioner will take a pap smear. She/he uses a long-stemmed cotton swab to collect a sample of cells in the cervix. Some women feel a slight cramping sensation when their cervix is touched. The collected cells are smeared onto a slide and sent to a lab for testing and examination. The pap smear is extremely important for spotting abnormalities in the cervix which may indicate infection or disease.
STD Testing
If you are sexually active, the practitioner will test for STDs. The gynecologist will swab the inside of the cervix with a long cotton swab. The speculum is then taken out of the vagina. The samples are sent to a laboratory for various STD testing. The tests will probably take a couple days. Ask when your results will be available so you can call. If you want to be tested for HIV, syphilis, genital herpes or hepatitis you need to have blood taken. They can do that as well, but you will need to ask since it is not usually routine.
Manual Exam
The second part of the pelvic exam is called the manual or bi-manual exam. The practitioner will insert one or two fingers into your vagina and press with her/his other hand on the outside of your lower abdomen. They will use a lubricant on their fingers so it is more comfortable. The person can then feel the uterus, fallopian tubes and ovaries, and check for any swelling or tenderness. Once the doctor is finished checking your uterus and ovaries, the exam is complete. The entire pelvic exam (the parts involving your vagina, cervix, uterus, and ovaries) takes 3 to 5 minutes to complete.
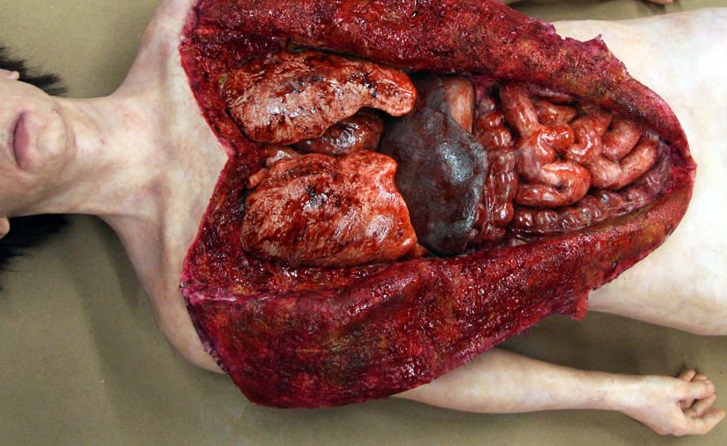
Watch that Full Female Body Medical Anatomy Autopsy

Watch that Female Recto-vaginal Exam Video

Dr Chris Steele demonstrates a breast examination on a live model. This shows how to check yourself for early signs of tumours, cysts and other symptoms of breast cancer.

Bimanual pelvic exam of a female, using two fingers inside the vagina and one hand on the outside of the abdomen.

Pelvic Exam Tutorial: Medical Video showing gynecological medical examination of the femal pelvis including bi-manual examintation

Pelvic Exam Video
https://www.youtube.com/watch?v=Uc6ZotU5mxA

Proctoscope rectal examination

-The cremasteric reflex test is considered positive if there is elevation of the testis in response to stroking the upper inner thigh. This reaction is typically absent in testicular torsion and boys under the age of 6 months. Although not completely reliable in older boys and adults, an absent cremasteric reflex is highly suggestive of torsion. Patients with epididymitis usually have a normal cremasteric reflex, with pain and swelling isolated to

childbirth twin baby

http://www.proctoscopeexam.com This is a demonstration of a proctoscope examination of the rectum.

Female Circumcision - FGM Female Genital Mutilation - female circumcision ختان الاناث - женское обрезание - circuncisão feminina - 女性割禮 - besnijdenis - babae pagtutuli - l'excision - κλειτοριδεκτομή - הנקבה מולה - sunat perempuan - circoncisione femminile - 女子割礼 - 여성 할례 - la circuncisión femenina - หญิง circumcision - kadın sünnet - жіноче обрізання For More read at World Health Organization web site : http://www.who.int/topics/female_genital_mutilation/en/index.html other sites : http://en.wikipedia.org/wiki/Female_genital_cutting

ectal exam is an internal examination of the rectum such as by a physician or other healthcare professional.
The digital rectal examination (DRE, Latin palpatio per anum or PPA) is a relatively simple procedure. The patient is placed in a position where the anus is accessible and relaxed (lying on the side, squatting on the examination table, bent over the examination table, etc). The physician inserts a gloved and lubricated finger into the rectum through the anus and palpates the insides.
The DRE is inadequate as a screening tool for colorectal cancer because it examines less than 10% of the colorectal mucosa; colonoscopy is preferred. However, it's an important part of a general examination, as many tumors or other diseases are made manifest in the distal part of the rectum.
This examination may be used: * for the diagnosis of rectal tumors and other forms of cancer; * in males, for the diagnosis of prostatic disorders, notably tumors and benign prostatic hyperplasia; * for the diagnosis of appendicitis or other examples of an acute abdomen (i.e. acute abdominal symptoms indicating a serious underlying disease); * for the estimation of the tonicity of the anal sphincter, which may be useful in case of fecal incontinence or neurologic diseases, including traumatic spinal cord injuries; * in females, for gynecological palpations of internal organs * for examination of the hardness and color of the feces (ie. in cases of constipation, and fecal impaction); * prior to a colonoscopy or proctoscopy. * to evaluate haemorrhoids
The DRE is frequently combined with an FOBT (fecal occult blood test), which may be useful for diagnosing the etiology of an anemia and/or confirming a gastrointestinal bleed.
Sometimes proctoscopy may also be part of a rectal examination.

CORRECTION: After review of this video, it is clear that this video is of a baby who is near full term (40 weeks) based on the size. Late trimester "abortions" are defined only to viability of a baby (24 weeks) A 24 week baby is much smaller than this baby shown and by definition this is not a late "abortion" procedure. The proper labeling of this video should be management of a deceased breech baby with "head entrapment" as this was almost certainly a naturally occuring delivery and an OB nightmare (Reviewed by Dr. Frederick Bright)

Orgasmic childbirth is a new variant of water birth delivery.
Maneuver to Correct Shoulder Dystocia Birth

A great video showing the multiple presentations of the baby which the doctor may encounter while delivery like breech presentation..etc

According to a recent study, most people's sexual romps last about 1.5–7 minutes. But, as Dr. Harry Fisch writes in his new book The New Naked: The Ultimate Sex Education for Grownups, 45 percent of men come in two minutes or less, leaving their female partners orgasmless. Here are some ways to extend your man's sexual stamina, and more likely have an orgasm yourself in the process.

Gynecological Examination
