- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

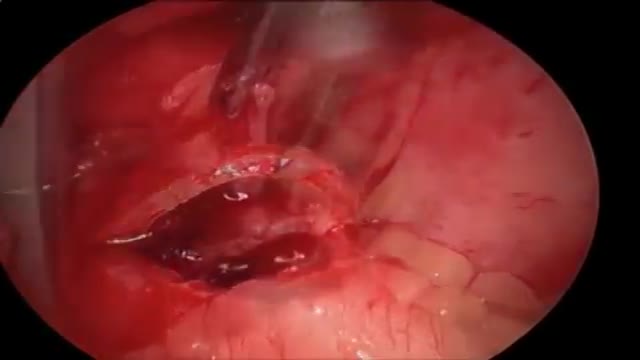
High volume sinus irrigation!

Peritoneal dialysis (per-ih-toe-NEE-ul die-AL-uh-sis) is a way to remove waste products from your blood when your kidneys can no longer do the job adequately. A cleansing fluid flows through a tube (catheter) into part of your abdomen and filters waste products from your blood. After a prescribed period of time, the fluid with filtered waste products flows out of your abdomen and is discarded. Peritoneal dialysis differs from hemodialysis, a more commonly used blood-filtering procedure. With peritoneal dialysis, you can give yourself treatments at home, at work or while traveling. Peritoneal dialysis isn't an option for everyone wit

MRI of Fetal Brain Development

Watch that video of Removing Gauze From a Spider's Bite
Alzheimer Disease Effects
http://endyourdepression.plus101.com ---Depression Alternative Medicine Remedies. Learn more about your own, unique depression symptoms and pin-point exactly which type of depression you are suffering from. Accurately discover what is causing your depression... and why it keeps coming back no matter which drugs you take or which treatments you try. Uncover the simple methods that allow you to switch your mind away from depression and towards real happiness. Gain real insight into why most depression treatments only make your symptoms worse. Depression Alternative Medicine Remedies depressive major disorder symptoms signs medication treatment clinical causes anxiety teen help hurts self test medicine antidepression types anxiety severe

At URBN Dental, we offer the best dental services and highest quality care for your gum tissue health. Proper flossing techniques prevent your gum tissue from swelling, which often occurs from food and debris catching between your teeth. A routine dental cleaning every 6 months is recommended to maintain gum tissue health. Skipping bi annual checkups and improper flossing techniques often lead to periodontal disease which usually require a dental deep cleaning to undo tissue damage.
Saddle pulmonary embolism (PE) is a form of large pulmonary thrombo-embolism that straddles the main pulmonary arterial trunk at its bifurcation. Its incidence among patients diagnosed with PE was found to be approximately 2.6%.

Watch that video to see How Snake Poison Coagulates Human Blood
Type 2 Diabetes Animation 3D
How to Know If You Have Diabetes

This video: Pancreatic cancer begins in the tissues of your pancreas — an organ in your abdomen that lies horizontally behind the lower part of your stomach. Your pancreas secretes enzymes that aid digestion and hormones that help regulate the metabolism of sugars. Pancreatic cancer often has a poor prognosis, even when diagnosed early. Pancreatic cancer typically spreads rapidly and is seldom detected in its early stages, which is a major reason why it's a leading cause of cancer death. Signs and symptoms may not appear until pancreatic cancer is quite advanced and complete surgical removal isn't possible.

Ultrasound-guided internal jugular cannulation
Providing information on the Atherosclerosis and its complex biological process: it is the idea of this medical video dedicated to the prevention of the cardiovascular risks of diseases.

Check out our new website http://www.evanshealthlab.com/
Follow Dr. Mike for new videos! http://twitter.com/docmikeevans
Dr. Mike Evans is founder of the Health Design Lab at the Li Ka Shing Knowledge Institute, an Associate Professor of Family Medicine and Public Health at the University of Toronto, and a staff physician at St. Michael's Hospital.
Written and Narrated by Dr. Mike Evans
Executive Producer, Dr. Mike Evans
Illustrations by Liisa Sorsa
Produced, Directed, and Photographed by Nick De Pencier
Editor, David Schmidt
Story/Graphic Facilitator, Disa Kauk
Production Assistant, Chris Niesing
Director of Operations, Mike Heinrich
©2014 Michael Evans and Reframe Health Films Inc.
The pituitary is a small gland found inside the skull just below the brain and above the nasal passages, which are above the fleshy back part of the roof of the mouth (known as the soft palate). The pituitary sits in a tiny bony space called the sella turcica. The nerves that connect the eyes to the brain, called the optic nerves, pass close by it.
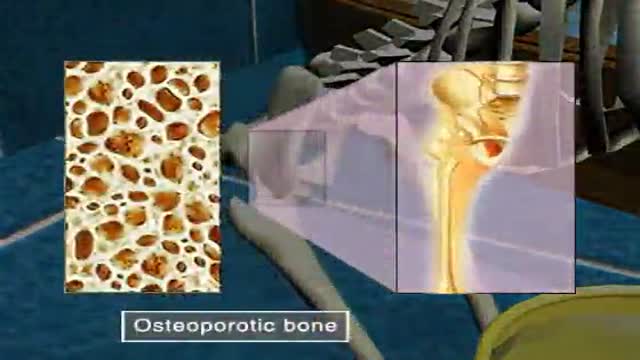
Osteoporosis

How to Know If You Have a Serious Knee Injury or Problem
Youtube Channel: https://www.youtube.com/user/physicaltherapyvideo
Website: https://bobandbrad.com/
Bob & Brad discuss how to know if you have a serious knee injury. They show you what to look for and what you should do.
This Week's Giveaway:
This month we are giving away a grand prize of a Sleepovation mattress and two pillows!
BONUS: 2 runners-up will receive a Sleepovation pillow!
December Giveaway link: https://shrsl.com/2ob0e
Purchase Mattress: http://shrsl.com/1n2e2
Purchase Pillow: http://shrsl.com/1xch4
Discount: Make sure to use the discount code FAMOUSPT to receive 15% off of your purchase of a mattress or use FAMOUSPTPIL for 25% off of their pillows! This is the biggest discount of the year!
Sleepovation will reimburse winners of the giveaway if they have already purchased, so no need to wait to buy Bob & Brad's favorite mattress and pillow!
Our videos offer the best "get fit , stay healthy, and pain-free" information directed toward people 0 to 101 years old. Physical Therapists Bob Schrupp and Brad Heineck have over 50 years of combined. We try to add a twist of our humor into each video in our quest to be the "Most Famous Physical Therapists on the Internet" In our opinion of course!!! Subscribe to us now and join the fun. Not only will these videos provide outstanding health information on treating yourself at home, we also do product reviews.
For our favorite products on Amazon click on this link: https://www.amazon.com/shop/physicaltherapyvideo
Visit us on our other social media platforms:
Website: https://bobandbrad.com/
Facebook: https://www.facebook.com/BobandBrad/
Instagram: https://www.instagram.com/officialbobandbrad/
Twitter: https://twitter.com/ptfamous
Bob and Brad’s Products:
Grip and Forearm Strengthener: https://store.bobandbrad.com
Wall Anchor: https://store.bobandbrad.com
Booyah Stik: https://store.bobandbrad.com
Knee Glide: https://store.bobandbrad.com
Fit Glide: https://store.bobandbrad.com
Massage Gun: https://amzn.to/36pMekg
Hanging Handles: https://amzn.to/2RXLVFF
Resistance Bands: https://amzn.to/36uqnbr
Pull Up Bands: https://amzn.to/3qmI4Rv
If you order from the Bob and Brad Store Links, you will receive 15% off your purchase.
Check out our shirts, mugs, bags and more in our Bob and Brad merchandise shop here: https://shop.spreadshirt.com/bob-brad
Bob & Brad Amazon Store: https://amzn.to/2RTSLLh
Other Products We Love: https://www.amazon.com/shop/physicaltherapyvideo?listId=3581Z1XUVFAFY
Check out The Bob & Brad Crew on YouTube by clicking here: https://www.youtube.com/c/thebobbradcrew
Want to help translate our videos? We would so love the help! http://www.youtube.com/timedtext_cs_panel?c=UCmTe0LsfEbpkDpgrxKAWbRA&tab=2
Medical Disclaimer All information, content, and material of this website is for informational purposes only and are not intended to serve as a substitute for the consultation, diagnosis, and/or medical treatment of a qualified physician or healthcare provider.
Affiliate disclaimer: Keep in mind that we may receive commissions when you click our links and make purchases. However, this does not impact our reviews and comparisons. We are highly selective in our products and try our best to keep things fair and balanced in order to help you make the best choice for you.

Add Me on
Instagram-https://instagram.com/_dialysi....s_therapist?igshid=Y
Telegram-https://t.me/dialysistherapist
Dialysis
Dialysis technician
Dialysis nurse
Kidney dialysis
Hemolysis
Dialysis technology
Dialysis therapist
Dialysis technician vacancy
Dialysis technician salary
Dialysis scope
Dialysis course scope
B.sc dialysis scope
Salary of dialysis technician
Role of dialysis technician
Salary of dialysis technician in india
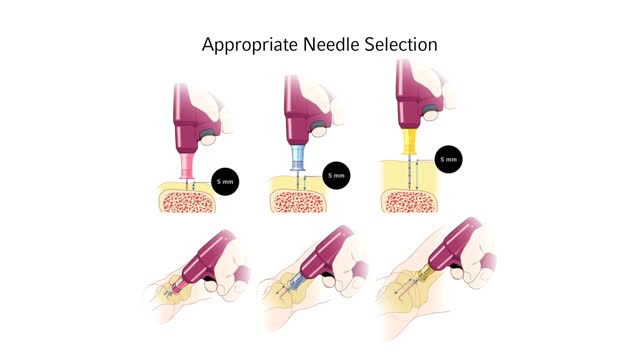
Infant Child Needle Selection and Insertion Technique Animation Video
