- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

New flu vaccines are released every year to keep up with rapidly adapting flu viruses. Because flu viruses evolve so quickly, last year's vaccine may not protect you from this year's viruses. After vaccination, your immune system produces antibodies that will protect you from the vaccine viruses.
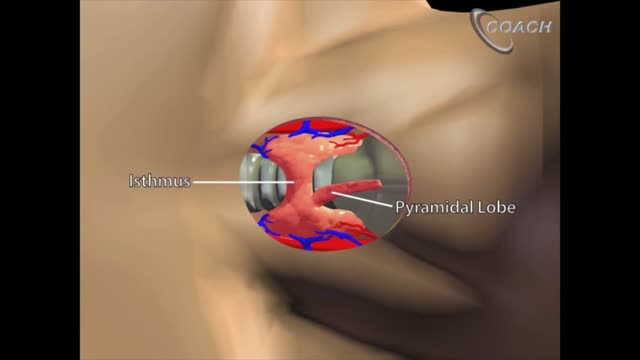
Minimally invasive open thyroidectomy (MIT) is similar to conventional thyroidectomy in its surgical approach. The major difference is the length of the neck incision. A smaller incision improves cosmesis and reduces discomfort. Typically, a skin incision less than 6 cm is considered minimally invasive. The remainder of the procedure is exactly the same as is used in conventional thyroidectomy. Adaptations to this technique include transection rather than lateral retraction of the strap muscles (the Sofferman technique). [1]
Invasive intracranial pressure monitoring. The most common surgically placed monitors for ICP measurement are intraventricular catheters (external ventricular drain [EVD] or a ventriculostomy drain) and fiberoptic ICP monitors implanted into the parenchyma of the brain.

Insert the needle into the rubber stopper of the insulin bottle. Push the plunger down to inject air into the bottle (this allows the insulin to be drawn more easily). Leave the needle in the bottle. Turn the bottle and syringe upside-down.

Broken or Dislocated Ankle Joint

Management of postpartum hemorrhage at vaginal delivery. The approach to treatment of postpartum hemorrhage (PPH) differs somewhat depending on the cause and whether hemorrhage occurs after a vaginal birth or after a cesarean delivery.
Pancreatic Auto Islet Transplantation is a procedure used to maintain insulin production and secretion in patients with chronic pancreatitis that are undergoing a total pancreatectomy, or removal of the entire pancreas. When all other medical therapies fail to control the pain, removal of the pancreas may be an option; however it can leave a person diabetic, which means that the body can no longer control blood sugar levels, and will require intensive testing of blood sugar and injections of insulin. The pancreas is an organ, located in the upper abdominal cavity, behind the stomach, liver and colon. Within the pancreas, specialized clusters of cells known as islets produce insulin, which maintain healthy blood sugar levels. The pancreas also produces enzymes to help digest food. In order to alleviate pain and maintain insulin production, the pancreas is removed from the body, processed and the islets are harvested. Once the pancreas is removed, it is placed in a solution and put into a machine where the pancreas is digested. The islets are then infused into the patient’s liver. Within a short time, the islets are expected to start producing insulin. In 80% of patients, the pain from pancreatitis is relieved by a total pancreatectomy. Over time, some patients may be diabetic and will need to take insulin to maintain healthy blood sugar levels. All patients will take pancreatic enzymes to help digest food after surgery.
This could be caused by an infection, food poisoning, parasites, Crohn's disease, or reduced blood flow in the colon. Hemorrhoids are another common cause of GI or rectal bleeding. A hemorrhoid is an enlarged vein in your rectum or anus. These enlarged veins can rupture and bleed, causing rectal bleeding.

Controlled studies on treatment of catscratch disease (CSD) are lacking. Thus, treatment recommendations are based on case reports, reviews, a single controlled trial, and anecdotal data. Practice guidelines for the diagnosis and management of skin and soft-tissue infections, including CSD, have been established.Oct 19, 2016
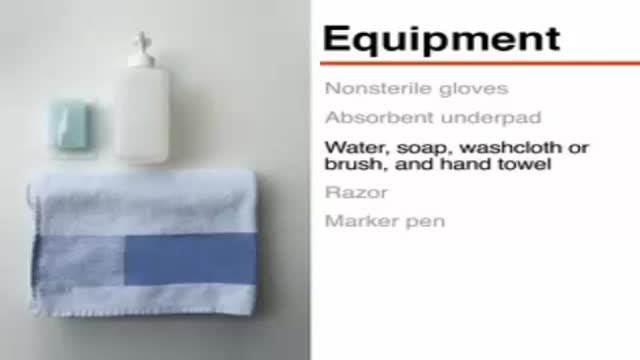
Wash your hands thoroughly with soap and water before and after treating the wound. Wash the area with mild soap and running water to reduce the risk of infection. Pat dry. Apply antibiotic ointment and cover with a clean bandage or sterile dressing. Antibiotic prophylaxis should be considered, especially if there is a high risk of infection, such as with cat bites, with puncture wounds, with wounds to the hand, and in persons who are immunosuppressed. Amoxicillin/clavulanate is the first-line prophylactic antibiotic.

Breast abscesses are often linked to mastitis – a condition that causes breast pain and swelling (inflammation), and usually affects women who are breastfeeding. Infections can occur during breastfeeding if bacteria enter your breast tissue, or if the milk ducts (tiny tubes) become blocked. This can cause mastitis which, if not treated, can result in an abscess forming. Women who aren't breastfeeding can also develop mastitis if bacteria enter the milk ducts through a sore or cracked nipple, or a nipple piercing. White blood cells are sent to attack the infection, which causes tissue at the site of the infection to die. This creates a small, hollow area that fills with pus (an abscess).
IVC filter is placed to prevent fatal Pulmonary Embolism due to Deep Venous Thrombosis (DVT). This particular patient had extensive DVT of Ilio-Femoral veins leading to massive swelling of left lower limb. The IVC filter was inserted via the Right Femoral Vein. This case was the first IVC filter placement of North Bengal and adjoining areas.

Colonoscopy is a test that allows your doctor to look at the inner lining of your large intestine (rectum and colon). He or she uses a thin, flexible tube called a colonoscope to look at the colon. A colonoscopy helps find ulcers, colon polyps, tumors, and areas of inflammation or bleeding.

If you are self-conscious because you have missing teeth, wear dentures that are uncomfortable or don't want to have good tooth structure removed to make a bridge, talk to your dentist to see if dental implants are an option for you. Dental implants are a popular and effective way to replace missing teeth and are designed to blend in with your other teeth. They are an excellent long-term option for restoring your smile. In fact, the development and use of implants is one of the biggest advances in dentistry in the past 40 years. Dental implants are made up of titanium and other materials that are compatible with the human body. They are posts that are surgically placed in the upper or lower jaw, where they function as a sturdy anchor for replacement teeth.

Most people have general anesthesia right before surgery. This means you will be asleep and pain-free. Other kinds of anesthesia, like regional anesthesia or a block, may also be used for this surgery. The tissue to replace your damaged ACL will come from your own body or from a donor. A donor is a person who has died and chose to give all or part of his or her body to help others. Tissue taken from your own body is called an autograft. The two most common places to take tissue from are the knee cap tendon or the hamstring tendon. Your hamstring is the muscle behind your knee. Tissue taken from a donor is called an allograft. The procedure is usually performed with the help of knee arthroscopy. With arthroscopy, a tiny camera is inserted into the knee through a small surgical cut. The camera is connected to a video monitor in the operating room. Your surgeon will use the camera to check the ligaments and other tissues of your knee. Your surgeon will make other small cuts around your knee and insert other medical instruments. Your surgeon will fix any other damage found, and then will replace your ACL by following these steps: The torn ligament will be removed with a shaver or other instruments. If your own tissue is being used to make your new ACL, your surgeon will make a larger cut. Then, the autograft will be removed through this cut. Your surgeon will make tunnels in your bone to bring the new tissue through. This new tissue will be in the same place as your old ACL. Your surgeon will attach the new ligament to the bone with screws or other devices to hold it in place. As it heals, the bone tunnels fill in. This holds the new ligament in place. At the end of the surgery, your surgeon will close your cuts with sutures (stitches) and cover the area with a dressing. You may be able to view pictures after the procedure of what the doctor saw and what was done during the surgery.

Application of collagen membrane GENIX IT. Derived entirely from pericardium of animal origin (Genix IT - Genix EGI), they are used to accelerate tissue...
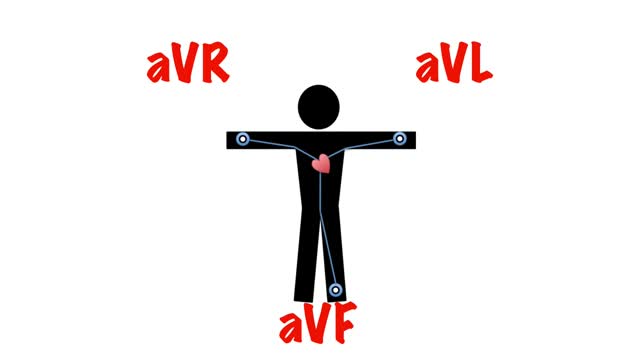
It then spreads down the bundle of his and then purkinje fibres to cause ventricular contraction. So when viewing the heart from the front, the direction of depolarisation is 11 o'clock to 5 o'clock. The general direction of depolarisation is known as the cardiac axis.

Why You’re Attracted To Certain People
http://vitiligo-home-remedies.plus101.com ---- white spots on skin, small white spots on face, what causes white spots on skin, vitiligo. The Link Between Vitiligo and Auto Immune Disorders. If you suffer with Vitiligo, a condition that strips your skin of its natural pigment or coloring, the odds are good that you are also battling some sort of autoimmune disorder. It took years for doctors to connect the two disorders, but recent research shows that at least 20 percent of Vitiligo suffers also get autoimmune thyroid disease, and that's juts the beginning. Many more suffer a multitude of other disorders. Until recently, the link between the Vitiligo and autoimmune problems were not clear. Doctors seemed to see a link, but nothing substantial could be proven. Until now. In march 2013, The National Institute's of Health's National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) announced an amazing discovery: a connection between a specific gene named NALP1, Vitiligo and a host of autoimmune diseases including thyroid disease, pernicious anemia, rheumatoid arthritis, lupus and Addison's Disease. According to lead researcher, Richard Spritz M.D., the discovery of this gene may make newer, more effective Vitiligo treatments possible within the next few years. But that's not all. It will also be able to help treat certain auto immune disorders. By finding ways to block the inflammatory response of the NALP1 gene, doctors may some day be able to cure certain autoimmune disorders. A long-term solution for vitiligo should address the internal causes of vitiligo by tackling all vitiligo contributing factors. Only by controlling the nutritional, hormonal, psychological and environmental triggers of vitiligo, using a multidimensional and holistic approach to healing you can reverse the "internal vitiligo environment"- the only, safe, natural and effective way you could ever achieve lasting vitiligo freedom. More Info: http://vitiligo-home-remedies.plus101.com
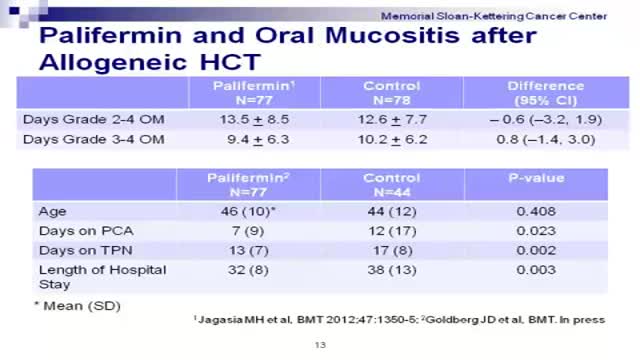
Graft-versus-host disease (GVHD) is a common complication after an allogeneic transplant, a transplant in which cells from a family member, unrelated donor or cord blood unit are used. In GVHD, the immune cells from the donated marrow or cord blood (the graft) attack the body of the transplant patient (the host).
