Top videos

🔥 Multivitamins for Men: https://lynxshort.com/Multivitamins-for-Men
✨ Multivitamins for Women: https://lynxshort.com/Multivitamins-for-Women
⭐ Multivitamins for Kids: https://lynxshort.com/Multivitamins-for-Kids
📙 Book of the Day 📚 https://lynxshort.com/Book-of-the-Day
This is one of the most interesting medical topics to discuss. What are the responsibilities of a doctor? What are the basic skills a doctor needs to have? and what are the responsibilities of a doctor?
**** CONNECT ****
- " Medical Videos " Android application on Google Play store:
https://play.google.com/store/....apps/details?id=com.
https://healthusher.com
https://www.facebook.com/MedicalVideosAnimated
https://www.instagram.com/medical_videos1
👉 Support Us to Help Us Continue Making Videos.. Thanks in Advance :)
- Via PayPal: https://www.paypal.me/medicalvideos
- Via Patreon: https://www.patreon.com/medicalvideosanimated
- The creator:
Pharmacist. Alaa Nasr
#MedicalVideosAnimated
Affiliate Disclaimer: This video and description contains affiliate links, which means that if you click on one of the product links, I'll receive a small commission. This is at no extra cost to you and in many cases include exclusive discounts where applicable. This helps support the channel and allows me to continue to make free videos like this. Thank you for the support!

This video shows you how to examine the hand and wrist and how to identify common causes of pain.
This video clip is part of the FIFA Diploma in Football Medicine and the FIFA Medical Network. To enrol or to find our more click on the following link http://www.fifamedicalnetwork.com
The Diploma is a free online course designed to help clinicians learn how to diagnose and manage common football-related injuries and illnesses. There are a total of 42 modules created by football medicine experts. Visit a single page, complete individual modules or finish the entire course.
The network provides the opportunity for clinicians around the world to meet and share ideas relating to football medicine. Ask about an interesting case, debate current practice and discuss treatment strategies. Create a profile and log on to interact with other health professionals from around the globe.
This is not medical advice. The content is intended as educational content for health care professionals and students. If you are a patient, seek care of a health care professional.

The thyroid gland lies in the midline of the anterior neck, just caudal to the thyroid cartilage. To inspect the thyroid gland, the examiner stands in front of the patient. The examiner asks the seated patient to dorsiflex (extend) the neck and swallow a sip of water. Minor enlargement of the gland may only become apparent on inspection in this position. Palpation of the thyroid gland is typically performed with the examiner standing behind the patient. Both lobes and the isthmus of the thyroid gland should be palpated for any nodules or diffuse enlargement. Mobility of the thyroid gland with swallowing should be assessed with palpation. Nodules arising from the thyroid gland typically move with swallowing. A hard, fixed thyroid gland could indicate malignancy. If a central nodule is identified, the patient is asked to protrude the tongue. Upward movement of the central nodule on protrusion of the tongue indicates a thyroglossal cyst. Auscultation is performed at the superior poles of bilateral lobes as this is where the superior thyroid artery is most superficial and bifurcates into its terminal branches. A bilateral bruit over the superior poles suggests Graves disease. Examination of the thyroid gland is completed by palpating the regional cervical lymph nodes for any enlargement.
Subscribe to AMBOSS YouTube for the latest clinical examination videos, medical student interviews, study tips and tricks, and live webinars!
Free 5 Day Trial: https://go.amboss.com/amboss-YT
Instagram: https://www.instagram.com/amboss_med/
Facebook: https://www.facebook.com/AMBOSS.Med/
Twitter: https://twitter.com/ambossmed
Blog: https://blog.amboss.com/us
#AMBOSSMed #ClinicalExamination #USMLE

Elbow Exam - Orthopaedic OSCE - Clinical Skills - Dr Gill
The elbow examination is a core skill - in this video, we demonstrate how to perform an elbow EXAM for an Orthopaedic Clinical Skills OSCE, which should be one of the more accessible examination stations for medical students.
For a passing grade in your Clinical Skills OSCE, an elbow assessment should follow the LOOK, FEEL, MOVE approach
Initially looking for erythema, scars, swelling and position
Palpating the elbow - specifically the olecranon, medial and lateral epicondyles, and radial head for heat, oedema and crepitus
Finally assess range of movement with flexion and extension at the elbow, before determining for tennis and golfers' elbows
Watch further orthopaedic examinations for your OSCE revision:
The Elbow - Deep Dive
https://youtu.be/SX5buhtCVDw
The Spine Examination:
https://youtu.be/pJxMHa6SCgU
The Knee examination
https://youtu.be/oyKH4EYfJDM
The Hip examination
https://youtu.be/JC9GKq5nSdQ
The GALS examination
https://youtu.be/5qJaf7gW-B0 - Gait, Arms, Legs, Spine - GALS screen
------------
Please note that there is no ABSOLUTE way to perform a clinical examination. Different institutions and even clinicians will have differing degrees of variations - the aim is the effectively identify medically relevant signs.
However during OSCE assessments. Different medical schools, nursing colleges and other health professional courses will have their own preferred approach to a clinical assessment - you should concentrate on THEIR marks schemes for your assessments.
The examination demonstrated here is derived from Macleods Clinical Examination - a recognised standard textbook for clinical skills.
Some people viewing this medical examination video may experience an ASMR effect
#clinicalskills #Elbow #DrGill

The cardiac examination is one of the earliest clinical skills that medical students learn. As a junior doctor, the examination of the cardiovascular system can be almost a dreaded examination, as cardiac murmurs can literally take years of exposure in order to gain confidence with their identification through cardiac auscultation.
This video demonstrates not merely the examination of the heart, but the complete cardiovascular system including peripheries.
I hope these clinical skill revision videos are helpful, please like and subscribe and join the community so that we can create more effective videos to help with your journey through medical school
#CardiacExam #ClinicalExamination #asmr

In this video, the viewer will learn the key aspects of the newborn physical exam, and how to distinguish between normal and abnormal findings.
Direct Links to chapters:
0:00-Intro
1:30-Head
3:49-Face
8:05-Neck
8:30-Chest
10:13-Abdomen
11:01-Groin
13:17-Extremities
14:05-Back
14:47-Neurologic
Please visit: www.openpediatrics.org
OPENPediatrics™ is an interactive digital learning platform for healthcare clinicians sponsored by Boston Children's Hospital and in collaboration with the World Federation of Pediatric Intensive and Critical Care Societies. It is designed to promote the exchange of knowledge between healthcare providers around the world caring for critically ill children in all resource settings. The content includes internationally recognized experts teaching the full range of topics on the care of critically ill children. All content is peer-reviewed and open access-and thus at no expense to the user.
For further information on how to enroll, please email: openpediatrics@childrens.harvard.edu
Please note: OPENPediatrics does not support nor control any related videos in the sidebar, these are placed by Youtube. We apologize for any inconvenience this may cause.

Respiratory Clinical Examination Demonstration - Clinical Skills OSCE Revision - Dr Gill
The respiratory examination is one of the three core clinical skills, respiratory, cardiac and abdominal examinations. In this video, we demonstrate how to perform a clinical examination of the RESPIRATORY SYSTEM for your medical school Clinical Skills OSCE. As the resp exam is sure a core skill when it comes to examining patients, students should assume that a respiratory assessment is a high yield station for any clinical exams or clinical assessments.
For a passing grade in your Clinical Skills OSCE, for resp examination follow the approach of:
- Inspection
- Palpation
- Percussion
- Auscultation
HOWEVER, a respiratory examination OSCE station does not just involve auscultating the lungs, this video also demonstrates some of the specialised examination techniques required in examining patients such as tactile vocal resonance, and checking the JVP which may be seen to be elevated in pulmonary hypertension
Coughs, colds and general concerns about the chest are a common reason for patients to see a doctor, and in any speciality is probably the most commonly performed patient examination
This video has two other respiratory system focused videos associated with it:
https://youtu.be/-Pm1SZyke-M - How to take a respiratory history
https://youtu.be/KFcXXn2aBPg - Understanding the techniques of the respiratory examination
Performed by Dr James Gill
------------
Please note that there is no ABSOLUTE way to perform a clinical examination. Different institutions and even clinicians will have differing degrees of variations - the aim is the effectively identify medically relevant signs.
However during OSCE assessments. Different medical schools, nursing colleges and other health professional courses will have their own preferred approach to a clinical assessment - you should concentrate on THEIR marks schemes for your assessments.
The examination demonstrated here is derived from Macleods Clinical Examination - a recognised standard textbook for clinical skills.
Some people may experience an ASMR effect from watching medical clinical examination videos
#clinicalskills #respiratoryexamination #DrJamesGill #asmr

Lesson on clinical examination of a scaphoid fracture and assessment of the anatomic snuffbox. The scaphoid bone is one of the carpal bones of the wrist. A scaphoid fracture is important to rule out due to risk of avascular necrosis, which is a compromise of bone vasculature leading to death of the bone. Scaphoid fractures can occur with a FOOSH injury. In this lesson, we discuss the clinical assessment to rule out a scaphoid fracture, including assessing and localizing the anatomic snuffbox.
If you find this lesson helpful, please consider liking, subscribing, and clicking the notification bell to help support this channel and stay up-to-date on future lessons.
*Subscribe for more free medical lessons* https://www.youtube.com/channe....l/UCFPvnkCZbHfBvV8Ap
-------------------------------------------------------------------------------------------------------------
For books and more information on these topics
https://www.amazon.com/shop/jjmedicine
Support future lessons (and get other cool stuff) ➜ https://www.patreon.com/jjmedicine
Follow me on Twitter! ➜ https://twitter.com/JJ_Medicine
Come join me on Facebook! ➜ https://www.facebook.com/JJ-Me....dicine-1006426481611
Start your own website with BlueHost ➜ https://www.bluehost.com/track/jjmedicine/
Check out the best tool to help grow your YouTube channel (it’s helped me!)
https://www.tubebuddy.com/jjmedicine
-------------------------------------------------------------------------------------------------------------
Check out some of my other lessons.
Medical Terminology - The Basics - Lesson 1:
https://www.youtube.com/watch?v=04Wh2E9oNug
Fatty Acid Synthesis Pathway:
https://www.youtube.com/watch?v=WuQS_LpNMzo
Wnt/B Catenin Signaling Pathway:
https://www.youtube.com/watch?v=NGVP4J9jpgs
Upper vs. Lower Motor Neuron Lesions:
https://www.youtube.com/watch?v=itNd74V53ng
Lesson on the Purine Synthesis and Salvage Pathway:
https://www.youtube.com/watch?v=e2KFVvI8Akk
Gastrulation | Formation of Germ Layers:
https://www.youtube.com/watch?v=d6Kkn0SECJ4
Introductory lesson on Autophagy (Macroautophagy):
https://www.youtube.com/watch?v=UmSVKzHc5yA
Infectious Disease Playlist
https://www.youtube.com/playli....st?list=PLRjNoiRtdFw
Dermatology Playlist
https://www.youtube.com/playli....st?list=PLRjNoiRtdFw
Pharmacology Playlist
https://www.youtube.com/playli....st?list=PLRjNoiRtdFw
Hematology Playlist
https://www.youtube.com/playli....st?list=PLRjNoiRtdFw
Rheumatology Playlist
https://www.youtube.com/playli....st?list=PLRjNoiRtdFw
Endocrinology Playlist
https://www.youtube.com/playli....st?list=PLRjNoiRtdFw
Nephrology Playlist
https://www.youtube.com/playli....st?list=PLRjNoiRtdFw
----------------------------------------------------------------------------------------------------
**MEDICAL DISCLAIMER**: JJ Medicine does not provide medical advice, and the information available on this channel does not offer a diagnosis or advice regarding treatment. Information presented in these lessons is for educational purposes ONLY, and information presented here is not to be used as an alternative to a healthcare professional’s diagnosis and treatment of any person/animal.
Only a physician or other licensed healthcare professional are able to determine the requirement for medical assistance to be given to a patient. Please seek the advice of your physician or other licensed healthcare provider if you have any questions regarding a medical condition.
----------------------------------------------------------------------------------------------------
*Although I try my best to present accurate information, there may be mistakes in this video. If you do see any mistakes with information in this lesson, please comment and let me know.*
I am always looking for ways to improve my lessons! Please don't hesitate to leave me feedback and comments - all of your feedback is greatly appreciated! :) And please don't hesitate to send me any messages if you need any help - I will try my best to be here to help you guys :)
Thanks for watching! If you found this video helpful, please like and subscribe!
JJ

Surgery 855 Examination of Hernia History Case Inspection Leg raising test Inguinal clinical feature
External ring Invagination
Internal ring occlusion test
History Inspection Palpation
taxis
Zieman


MRCPCH Clinical Revision - more videos at http://mrcpch.paediatrics.co.uk
Revise for your MRCPCH Clinical exam, with videos and high quality content created by the London Paediatrics Trainees Committee.
Video Credits: Dr Caroline Fertleman, Dr Hermione Race, Dr Camilla Sen, Dr Chloe Macaulay, Dr Emma McLaren, Chris Knapp

#ComprehensiveClinicalClass
History, Examination and Management of Hernia
Mentor: Dr. Nishanth, Consultant Surgeon, Bengaluru.
THE WHITE ARMY
To make studies more interesting and enjoyable, we are constantly trying to share most important tables, charts, diagrams, mnemonics, scoring systems, diagnostic criterias, motivating quotes and other useful study materials on
ANDROID APP - All in 1 Free Medical Education App for Medicos
https://play.google.com/store/....apps/details?id=com.
INSTAGRAM PAGE
@the_whitearmy
https://www.instagram.com/the_whitearmy/
TELEGRAM GROUP
PDFs, PPTs and other study materials stored for easy, convenient access and download.
https://t.me/whitearmyofmedicos
Anyone interested to present clinical cases, willing to join whatsapp discussion group, can send a mail to whitearmyofmedicos@gmail.com
#StudyManiaInSocialMedia
#HelpOthersToHelpOurselves
#StudyEnjoyingEnjoyStudying
DISCLAIMER
THE WHITE ARMY does not own or claim to own any of the media used in the following video/stream. The media belong to their respective owners who may have copyright over them.The media have been taken from various sources and are used for medical educational purposes only. The following video/stream may contain images that may not be suitable for all audiences, viewer discretion is advised.

In this video, we show a sports hernia self treatment we give many of our clients. It is not the only part of treatment. Grabbing the skin around the region of the groin strain can reduce pain and stiffness with turning and twisting. Sports hernias are often misdiagnosed with hip labrum tears, hip impingement, adductor tendonitis and abdominal strains.
Want more information? We have a more detailed free webinar on our page here. https://bit.ly/37thtNF
Want some treatment or suggestions of exercises or stretches? Contact us! We have in-person and virtual sessions.
Costa Mesa CA 715-502-4243 www.p2sportscare.com
Sports Hernia Diagnosis
What Is A Sports Hernia?
A sports hernia is tearing of the transversalis fascia of the lower abdominal or groin region. A common misconception is that a sports hernia is the same as a traditional hernia. The mechanism of injury is rapid twisting and change of direction within sports, such as football, basketball, soccer and hockey.
The term “sports hernia” is becoming mainstream with more professional athletes being diagnosed. The following are just to name a few:
Torii Hunter
Tom Brady
Ryan Getzlaf
Julio Jones
Jeremy Shockey
If you follow any of these professional athletes, they all seem to have the same thing in common: Lingering groin pain. If you play fantasy sports, this is a major headache since it seems so minor, but it can land a player on Injury Reserve on a moments notice. In real life, it is a very frustrating condition to say the least. It is hard to pin point, goes away with rest and comes back after activity, but is hardly painful enough to make you want to stop. It lingers and is always on your mind. And if you’re looking for my step-by-step sports hernia rehab video course here it is.
One the best definitions of Sport hernias is the following by Harmon:
The phenomena of chronic activity–related groin pain that it is unresponsive to conservative therapy and significantly improves with surgical repair.”
This is truly how sports hernias behave in a clinical setting. It is not uncommon for a sports hernia to be unrecognized for months and even years. Unlike your typical sports injury, most sports medicine offices have only seen a handful of cases. It’s just not on most doctors’ radar. The purpose of this article is not only to bring awareness about sports hernias, but also to educate.
Will you find quick fixes in this article for sports hernia rehab?
Nope. There is no quick fix for this condition, and if someone is trying to sell you one, they are blowing smoke up your you-know-what.
Is there a way to decrease the pain related to sports hernias?
Yes. Proper rehab and avoidance of activity for a certain period of time will assist greatly, but this will not always stop it from coming back. Pain is the first thing to go and last thing to come. Do not be fooled when you become pain-free by resting it. Pain is only one measure of improvement in your rehab. Strength, change of direction, balance and power (just to name a few) are important, since you obviously desire to play your sport again. If you wanted to be a couch potato, you would be feeling better in no time. Watching Sports Center doesn’t require any movement.
Why is this article so long?
There is a lot of information on sports hernias available to you on the web. However, much of the information is spread out all over the internet and hard for athletes to digest due to complicated terminology. This article lays out the foundational terminology you will need to understand what options you have with your injury. We will go over anatomy, biomechanics, rehab, surgery, and even the fun facts. The information I am using is from the last ten years of medical research, up until 2016. We will be making updates overtime when something new is found as well. So link to this page and share with friends. This is the best source for information on sports hernias you will find.
Common Names (or Aliases?) for Sports Hernias
Sportsman’s Hernia
Athletic Pubalgia
Gilmore’s Groin
How Do You Know If You Have A Sports Hernia?
Typical athlete characteristics:
Male, age mid-20s
Common sports: soccer, hockey, tennis, football, field hockey
Motions involved: cutting, pivoting, kicking and sharp turns
Gradual onset
How A Sports Hernia Develops
Chronic groin pain typically happens over time, which is why with sports hernias, we do not hear many stories of feeling a “pop” or a specific moment of injury. It is the result of “overuse” mechanics stemming from a combination of inadequate strength and endurance, lack of dynamic control, movement pattern abnormalities, and discoordination of motion in the groin area.
#sportsherniadiagnosisselftreatment #sportshernia #california

We will show how to know if you have a sports hernia. These are a few tests you can do on your own. Lower abdominal pain and tightness that increases with twisting and kicking. Stretching and exercises tend to make the discomfort increase.
Want more info? We have a free webinar that covers hip, groin, adductor, lower abdominal strains and sports hernia diagnosis in detail. Use this link to get access. https://bit.ly/37thtNF
#sportshernia #hernia #hippain
To work with us, contact us using this link https://bit.ly/3zCBnzZ or call us 714-502-4243. We have online programs, virtual and in-person options.
Costa Mesa, CA www.p2sportscare.com
Option 1: Groin On-Demand Webinar https://bit.ly/37thtNF
Option 2: Video Guide https://bit.ly/33aLIqC
Option 3 (the best): Work With Us https://www.p2sportscare.com/
Sports Hernia Diagnosis
What Is A Sports Hernia?
A sports hernia is tearing of the transversalis fascia of the lower abdominal or groin region. A common misconception is that a sports hernia is the same as a traditional hernia. The mechanism of injury is rapid twisting and change of direction within sports, such as football, basketball, soccer and hockey.
The term “sports hernia” is becoming mainstream with more professional athletes being diagnosed. The following are just to name a few:
Torii Hunter
Tom Brady
Ryan Getzlaf
Julio Jones
Jeremy Shockey
If you follow any of these professional athletes, they all seem to have the same thing in common: Lingering groin pain. If you play fantasy sports, this is a major headache since it seems so minor, but it can land a player on Injury Reserve on a moments notice. In real life, it is a very frustrating condition to say the least. It is hard to pin point, goes away with rest and comes back after activity, but is hardly painful enough to make you want to stop. It lingers and is always on your mind. And if you’re looking for my step-by-step sports hernia rehab video course here it is.
One the best definitions of Sport hernias is the following by Harmon:
The phenomena of chronic activity–related groin pain that it is unresponsive to conservative therapy and significantly improves with surgical repair.”
This is truly how sports hernias behave in a clinical setting. It is not uncommon for a sports hernia to be unrecognized for months and even years. Unlike your typical sports injury, most sports medicine offices have only seen a handful of cases. It’s just not on most doctors’ radar. The purpose of this article is not only to bring awareness about sports hernias, but also to educate.
Will you find quick fixes in this article for sports hernia rehab?
Nope. There is no quick fix for this condition, and if someone is trying to sell you one, they are blowing smoke up your you-know-what.
Is there a way to decrease the pain related to sports hernias?
Yes. Proper rehab and avoidance of activity for a certain period of time will assist greatly, but this will not always stop it from coming back. Pain is the first thing to go and last thing to come. Do not be fooled when you become pain-free by resting it. Pain is only one measure of improvement in your rehab. Strength, change of direction, balance and power (just to name a few) are important, since you obviously desire to play your sport again. If you wanted to be a couch potato, you would be feeling better in no time. Watching Sports Center doesn’t require any movement.
Why is this article so long?
There is a lot of information on sports hernias available to you on the web. However, much of the information is spread out all over the internet and hard for athletes to digest due to complicated terminology. This article lays out the foundational terminology you will need to understand what options you have with your injury. We will go over anatomy, biomechanics, rehab, surgery, and even the fun facts. The information I am using is from the last ten years of medical research, up until 2016. We will be making updates overtime when something new is found as well. So link to this page and share with friends. This is the best source for information on sports hernias you will find.
Common Names (or Aliases?) for Sports Hernias
Sportsman’s Hernia
Athletic Pubalgia
Gilmore’s Groin
How Do You Know If You Have A Sports Hernia?
Typical athlete characteristics:
Male, age mid-20s
Common sports: soccer, hockey, tennis, football, field hockey
Motions involved: cutting, pivoting, kicking and sharp turns
Gradual onset
How A Sports Hernia Develops
Chronic groin pain typically happens over time, which is why with sports hernias, we do not hear many stories of feeling a “pop” or a specific moment of injury. It is the result of “overuse” mechanics stemming from a combination of inadequate strength and endurance, lack of dynamic control, movement pattern abnormalities, and discoordination of motion in the groin area.

Step in the Clinic with Dr. Pritesh Singh and get a practical insight into the Clinical Examination of Incisional Hernia.
Now Save Time with these Exam Relevant Clinical Videos & Waste None Studying Rare Cases.
Prepare with 2021 Dream Pack. It includes everything you need to ace Medical PG Entrance Exams. To enroll or know more visit: https://premium.prepladder.com/
=======================================================
To experience PrepLadder's excellent learning, download the app:
iOS: https://bit.ly/prepladderios
Android: https://bit.ly/prepladderandroid
Follow us on Social Media for all the latest updates:
Facebook: https://www.facebook.com/medic....al.pg.entrance.prepl
Instagram: https://www.instagram.com/prepladder_med
Subscribe to our YouTube channel and press the bell icon for more videos and regular updates: https://www.youtube.com/channe....l/UCdbMxSVAgPENqhYVe
#PrepLadder #ClinicalEssentials #PadhoWoChahiyeJo #DrPriteshSingh #Surgery #NEETPG #IncisionalHernia #2021DreamPack

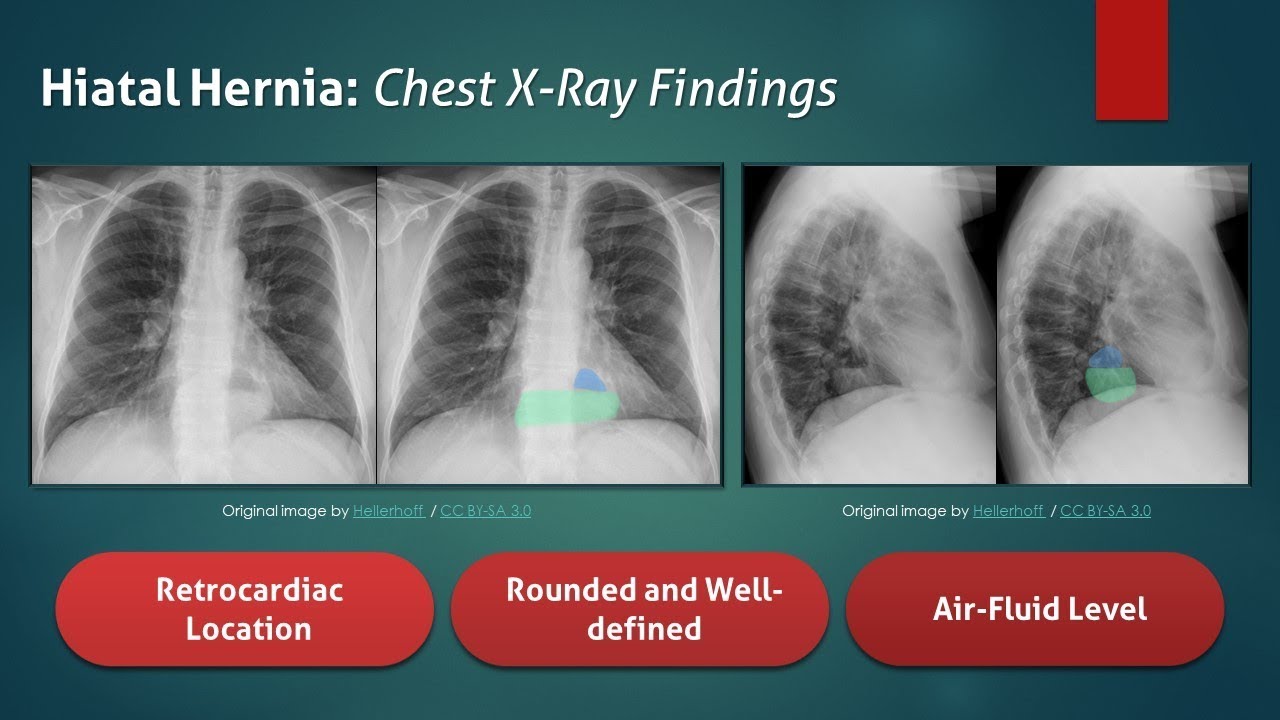
The typical radiograph is of a well-defined, rounded, retrocardiac opacity with an air-fluid level. In this image, the radiolucent gas is highlighted in blue, while the gastric contents are highlighted in the green. In many cases of hiatal hernia, there will not be an air bubble below the left hemidiaphragm. This is a relatively expected finding considering that the stomach is no longer in its usual position. The anatomical position of the herniated organ can be further elucidated on the lateral radiograph. Here we can see that the stomach is in the middle mediastinum posterior to the heart and above the diaphragm. Hiatal hernias can look similar to a retrocardiac lung abscess or another cavitary lesion, but it will change in size and shape between radiographs. Large hernias can shift the mediastinum to the right and result in a widening of the carinal angle. They can even give the appearance of cardiomegaly. In this radiograph, the cardiac silhouette is distinctly visible within the confines of the hiatal hernia. To review, a hiatal hernia on an AP chest radiograph typically appears as a round retrocardiac opacity with an air-fluid level.
🌐 Check out our website for more video lectures
https://www.med4vl.com
📺 Subscribe To My Channel and Get More Great Quizzes and Tutorials
https://www.youtube.com/channe....l/UC95TzSH1B_2EjaZMg
#FOAMrad #MedEd #radiology
Disclaimer: All the information provided by Medical Education for Visual Learners and associated videos are strictly for informational purposes only. It is not intended as a substitute for medical advice from your health care provider or physician. It should not be used to overrule the advice of a qualified healthcare provider, nor to provide advice for emergency medical treatment. If you think that you or someone that you know may be suffering from a medical condition, then please consult your physician or seek immediate medical attention.
Try our MULTIPLE CHOICE QUESTIONS and WATCH MORE VIDEOS at www.boxmedicine.com!
Inguinal and femoral hernias need not be confusing. In this tutorial you will be presented with colourful diagrams and animations to cover important areas, such as the anatomy of what goes on in these two conditions, the examination of groin hernias and a simple explanation of the difference between incarceration, strangulation and obstruction, in and amongst a systematic look at the clinical topic. More tutorials at www.boxmedicine.com.

Contact us to find out more http://www.londonvisionclinic.com/contact-us/ A video of an actual lasik eye surgery procedure taking place, using VisuMax and MEL 80 at the London Vision Clinic.
Visit http://www.londonvisionclinic.....com/are-you-suitable to find out more about the laser eye surgery process.

Purchase a license to download a non-watermarked copy of this video here: https://www.alilamedicalmedia.....com/-/galleries/all-
Voice by: Sue Stern.
©Alila Medical Media. All rights reserved.
Support us on Patreon and get FREE downloads and other great rewards: patreon.com/AlilaMedicalMedia
Perfect for patient education purposes.
All images/videos by Alila Medical Media are for information purposes ONLY and are NOT intended to replace professional medical advice, diagnosis or treatment. Always seek the advice of a qualified healthcare provider with any questions you may have regarding a medical condition.
LASIK, or "laser-assisted in situ keratomileusis," is the most commonly performed laser eye surgery to treat myopia, hyperopia and astigmatism. The goal of the treatment is to reshape the cornea to correct the refractive error of the eye.
The cornea is the transparent dome-shaped structure in front of the eye. The cornea refracts light and accounts for about two-thirds of the eye's total optical power. Altering the curvature of the cornea changes the way light rays enter the eye. As a result, the light rays can be focused properly onto the retina for clearer vision.
For nearsighted people, the laser is used to flatten the cornea. For farsighted people, the cornea is made steeper. For patients with astigmatism, the laser is used to smooth the irregularly-shaped cornea into a more regular shape.
The outer layer of the cornea - the epithelium – is capable of replacing itself within a few days after being damaged or removed. The deeper layer of the cornea – the stroma, on the contrary, is a permanent corneal tissue with very limited regenerative capacity. The stroma, if reshaped by a laser, will remain that way permanently.
In this procedure, a thin, circular "FLAP" is created in the surface of the cornea to gain access to the permanent corneal tissue. This can be done with a mechanical cutting tool called a microkeratome, OR, for a blade-free experience, by a femtosecond laser. An excimer laser is then used to remove some corneal tissue to reshape the cornea. Excimer laser uses cool ultraviolet light beams to vaporize microscopic amounts of tissue in a precise manner to accurately reshape the cornea. The excimer laser is computer-controlled and is programmed based on the patient’s refractive error. The flap is then laid back in place and is allowed to heal.
LASIK eye surgery is mostly painless and can be completed within minutes. Improved vision can usually be seen overnight.
PRK, or photorefractive keratectomy, was the first type of laser eye surgery for vision correction and is the predecessor to the popular LASIK procedure. In PRK, NO flap is created. Rather, the epithelial cells on the eye surface are simply removed. An excimer laser is then used to reshape the cornea just like it does in LASIK.
The vision correction outcomes of PRK surgery are comparable to those of LASIK, but the recovery period is longer. This is because the epithelium is completely removed in PRK and it takes a few days to regenerate. PRK patients also have more discomfort and haziness of vision in the first few days after the surgery. Improved vision also takes longer to achieve.
PRK does, however, offer certain advantages. Because PRK does not involve creation of a flap, which contains both epithelial and deeper stromal tissue, the entire thickness of the stroma is available for treatment. The treatment range is therefore higher. This is particularly useful for patients with high levels of myopia or for those whose cornea is too thin for LASIK. PRK is also free of flap-related complication risks.
