Video hàng đầu
First Head Transplant Surgery

Aspirin is used to reduce fever and relieve mild to moderate pain from conditions such as muscle aches, toothaches, common cold, and headaches. It may also be used to reduce pain and swelling in conditions such as arthritis. Aspirin is known as a salicylate and a nonsteroidal anti-inflammatory drug (NSAID).

Meet Christian, an incredible man born with no arms or legs who lives life to the fullest

atrial septal defect (ASD) is a hole in the wall between the two upper chambers of your heart (atria). The condition is present from birth (congenital). Small atrial septal defects may close on their own during infancy or early childhood. Large and long-standing atrial septal defects can damage your heart and lungs. Small defects may never cause a problem and may be found incidentally. An adult who has had an undetected atrial septal defect for decades may have a shortened life span from heart failure or high blood pressure that affects the arteries in the lungs (pulmonary hypertension). Surgery may be necessary to repair atrial septal defects to prevent complications
The urinary bladder is a hollow muscular organ that collects urine from the kidneys before disposal by urination. A hollow muscular, and distensible (or elastic) organ, the bladder sits on the pelvic floor. Urine enters the bladder via the ureters and exits via the urethra.

Work out the length of your average menstrual cycle. Day one is the first day of the menstrual period and the last day is the day before the next period begins. Ovulation happens about two weeks before the next expected period. So if your average menstrual cycle is 28 days, you ovulate around day 14.
This could be caused by an infection, food poisoning, parasites, Crohn's disease, or reduced blood flow in the colon. Hemorrhoids are another common cause of GI or rectal bleeding. A hemorrhoid is an enlarged vein in your rectum or anus. These enlarged veins can rupture and bleed, causing rectal bleeding.
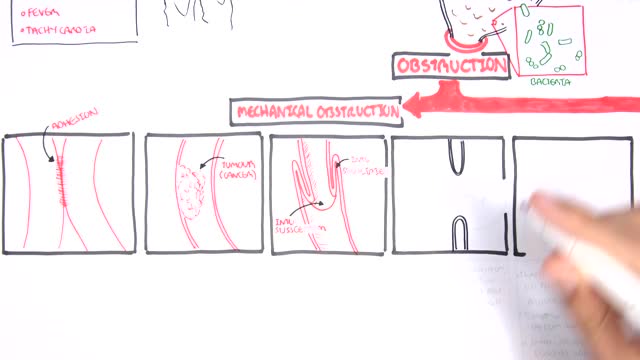
A bowel obstruction happens when either your small or large intestine is partly or completely blocked. The blockage prevents food, fluids, and gas from moving through the intestines in the normal way. The blockage may cause severe pain that comes and goes. This topic covers a blockage caused by tumors, scar tissue, or twisting or narrowing of the intestines. It does not cover ileus, which most commonly happens after surgery on the belly (abdominal surgery). What causes a bowel obstruction? Tumors, scar tissue (adhesions), or twisting or narrowing of the intestines can cause a bowel obstruction. These are called mechanical obstructions . In the small intestine, scar tissue is most often the cause. Other causes include hernias and Crohn's disease, which can twist or narrow the intestine, and tumors, which can block the intestine. A blockage also can happen if one part of the intestine folds like a telescope into another part, which is called intussusception.

Controlled studies on treatment of catscratch disease (CSD) are lacking. Thus, treatment recommendations are based on case reports, reviews, a single controlled trial, and anecdotal data. Practice guidelines for the diagnosis and management of skin and soft-tissue infections, including CSD, have been established.Oct 19, 2016

The heart is the body's engine room, responsible for pumping life-sustaining blood via a 60,000-mile-long (97,000-kilometer-long) network of vessels. The organ works ceaselessly, beating 100,000 times a day, 40 million times a year—in total clocking up three billion heartbeats over an average lifetime. It keeps the body freshly supplied with oxygen and nutrients, while clearing away harmful waste matter.

Ventral Hernia Repair

Cosmetic Eye and Eyelid Surgery

irregular, curved toenails. footwear that places a lot of pressure on the big toes, such as socks and stockings that are too tight or shoes that are too tight, narrow, or flat for your feet. toenail injury, including stubbing your toe, dropping something heavy on your foot, or kicking a ball repeatedly. poor posture. How can ingrowing toenails be prevented? Cut your nails straight across; do not cut them too short or too low at the sides. ... Keep your feet clean and dry. ... Avoid tight shoes and use cotton socks rather than synthetic. If you have diabetes, you should take extra care when cutting your nails:
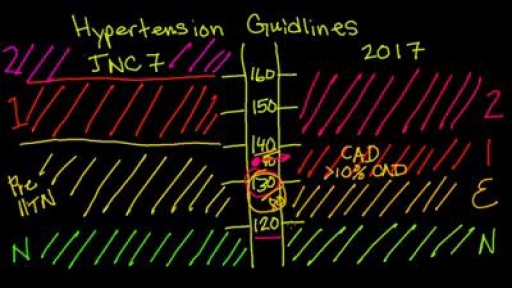
New 2017 Hypertension guidelines
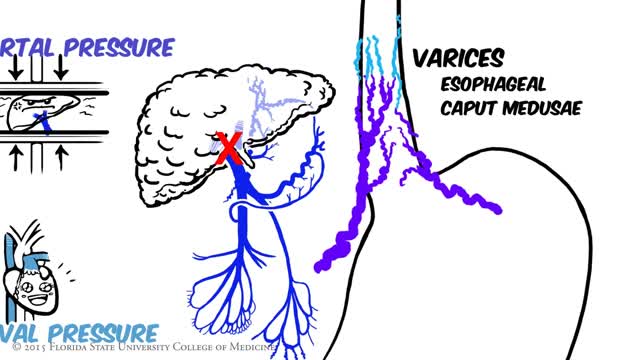
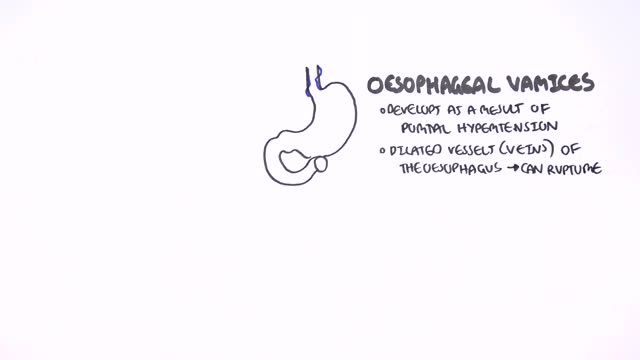
Portal hypertension is an increase in the blood pressure within a system of veins called the portal venous system. Veins coming from the stomach, intestine, spleen, and pancreas merge into the portal vein, which then branches into smaller vessels and travels through the liver.

Although the Apgar score was developed in 1952 by an anesthesiologist named Virginia Apgar, you also might hear it referred to as an acronym for: Appearance, Pulse, Grimace, Activity, and Respiration. The Apgar test is usually given to a baby twice: once at 1 minute after birth, and again at 5 minutes after birth.
Nephritis and Nephrotic Syndrome

Animation of Scarless Varicose Vein Treatment No Knife Endovenous Laser
Major signs and symptoms include enlargement of the liver and spleen (hepatosplenomegaly), a low number of red blood cells (anemia), easy bruising caused by a decrease in blood platelets (thrombocytopenia), lung disease, and bone abnormalities such as bone pain, fractures, and arthritis.

When taking oral corticosteroids longer term, you may experience: Clouding of the lens in one or both eyes (cataracts) High blood sugar, which can trigger or worsen diabetes. Increased risk of infections. Thinning bones (osteoporosis) and fractures. Suppressed adrenal gland hormone production
