Top Videos

This video shows you how to examine the hand and wrist and how to identify common causes of pain.
This video clip is part of the FIFA Diploma in Football Medicine and the FIFA Medical Network. To enrol or to find our more click on the following link http://www.fifamedicalnetwork.com
The Diploma is a free online course designed to help clinicians learn how to diagnose and manage common football-related injuries and illnesses. There are a total of 42 modules created by football medicine experts. Visit a single page, complete individual modules or finish the entire course.
The network provides the opportunity for clinicians around the world to meet and share ideas relating to football medicine. Ask about an interesting case, debate current practice and discuss treatment strategies. Create a profile and log on to interact with other health professionals from around the globe.
This is not medical advice. The content is intended as educational content for health care professionals and students. If you are a patient, seek care of a health care professional.
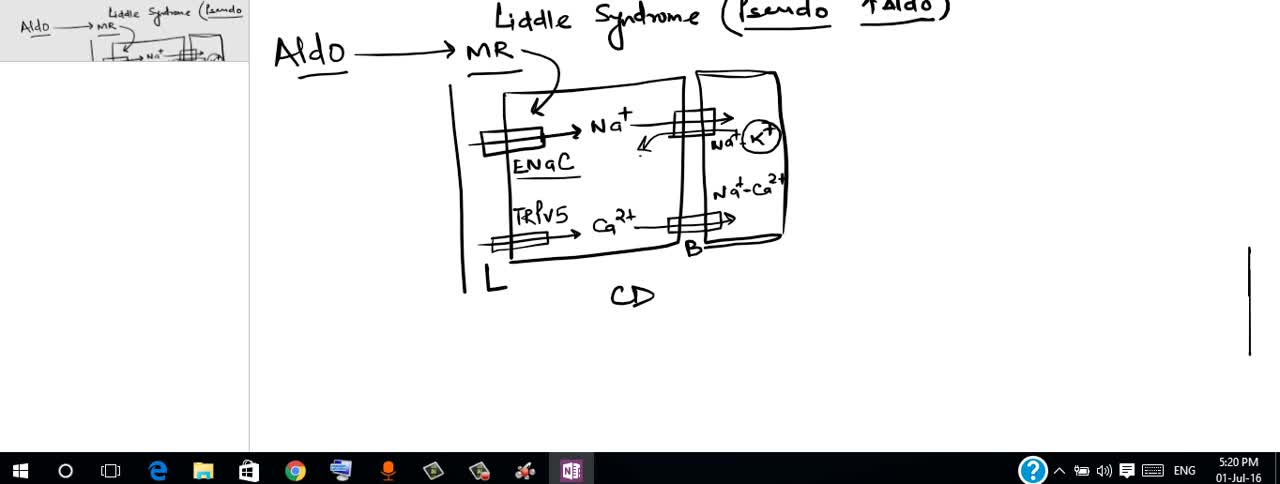
Liddle syndrome is an inherited form of high blood pressure (hypertension). This condition is characterized by severe hypertension that begins unusually early in life, often in childhood, although some affected individuals are not diagnosed until adulthood. Some people with Liddle syndrome have no additional signs or symptoms, especially in childhood. Over time, however, untreated hypertension can lead to heart disease or stroke, which may be fatal.

The da Vinci® Surgical System provides surgeons with an alternative to both traditional open surgery and conventional laparoscopy, putting a surgeon's hands at the controls of a state-of-the-art robotic platform. Our surgeons can perform even the most complex and delicate procedures through very small incisions with unmatched precision.

Watch that video of a Man's Arm Exploded Due to Illegal Muscles Injections

Shoulder Clinical Examination - Medical School Clinical Skills - Dr Gill
Personally, I find the shoulder examination the most complex examination possibly as there are so many variations and special tests. Some of which overlap and some will relate specifically to a patients presentation.
Often in a medical school syllabus, only select special tests will be used. In this shoulder exam demonstration, we include the Hawkins-Kennedy Test looking for impingement. This is dovetailed with examination for bicipital tendonitis as this is another possible cause of impingement type symptoms.
This shoulder upper limb exam follows the standard "Look, Feel, Move" orthopaedic exam approach, and overall order as set out in MacLeods Clinical Examination
Watch further orthopaedic examinations for your OSCE revision:
The Spine Examination:
https://youtu.be/pJxMHa6SCgU
Knee Examination
https://youtu.be/oyKH4EYfJDM
Hip Joint Clinical Examination
https://youtu.be/JC9GKq5nSdQ
________
Please note that there is no ABSOLUTE way to perform a clinical examination. Different institutions and even clinicians will have differing degrees of variations - the aim is the effectively identify medically relevant signs.
However during OSCE assessments. Different medical schools, nursing colleges, and other health professional courses will have their own preferred approach to a clinical assessment - you should concentrate on THEIR marks schemes for your assessments.
The examination demonstrated here is derived from Macleods Clinical Examination - a recognized standard textbook for clinical skills.
#ShoulderExamination #ClinicalSkills #DrGill

Ligation around a hemostatic Clamp

How to give Intramuscular (IM) injection

Physical Examination of the abdomen

This video: Blisters caused by friction or minor burns do not require a doctor's care. New skin will form underneath the affected area and the fluid is simply absorbed. Do not puncture a blister unless it is large, painful, or likely to be further irritated. The fluid-filled blister keeps the underlying skin clean, which prevents infection and promotes healing.

Perineal Protectomy for Rectal Prolapse
Transverse Colostomy Closure

Pilonidal disease with lateral extension. Follicle removal (Bascon's technique)

Pinch air out of the tip of the condom. Unroll condom all the way down the penis. After sex but before pulling out, hold the condom at the base. Then pull out, while holding the condom in place. Carefully remove the condom and throw it in the trash.

Cluster headaches, occur in cyclical patterns or clusters, are one of the most painful types of headache. A cluster headache commonly awakens you in the middle of the night with intense pain in or around one eye on one side of your head. Bouts of frequent attacks, known as cluster periods, can last from weeks to months, usually followed by remission periods when the headaches stop. During remission, no headaches occur for months and sometimes even years. Fortunately, cluster headache is rare and not life-threatening. Treatments can make cluster headache attacks shorter and less severe. In addition, medications can reduce the number of cluster headaches.
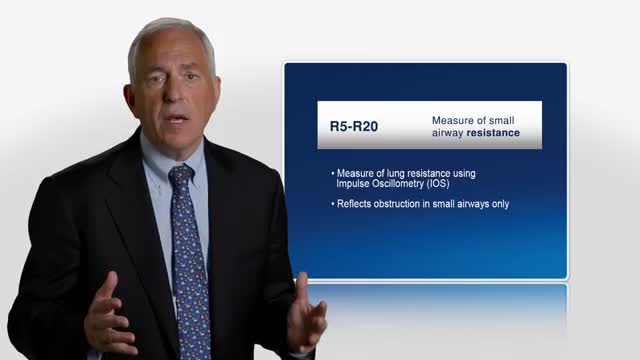
Asthma was originally described as an inflammatory disease that predominantly involves the central airways. Pathological and physiological evidence reported during the past few years suggests that the inflammatory process extends beyond the central airways to the peripheral airways and the lung parenchyma. The small airways are capable of producing T-helper-2 cytokines, as well as chemokines, and they have recently been recognized as a predominant site of airflow obstruction in asthmatic persons. The inflammation at this distal site has been described as more severe than large airway inflammation. These findings are of great clinical significance, and highlight the need to consider the peripheral airways as a target in any therapeutic strategy for treatment of asthma.
Renal artery stenosis is the narrowing of one or more arteries that carry blood to your kidneys (renal arteries). Narrowing of the arteries prevents normal amounts of oxygen-rich blood from reaching your kidneys. Your kidneys need adequate blood flow to help filter waste products and remove excess fluids. Reduced blood flow may increase blood pressure in your whole body (systemic blood pressure) and injure kidney tissue.

Laparotomy (opening and closing)

A walk through of an interactive about male to female sex reassignment surgery.

Gastrointestinal GI Drug Delivery
Repair of Anomalous Left Coronary Artery from the Pulmonary Artery (AlCAPA) in an Adult
