- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

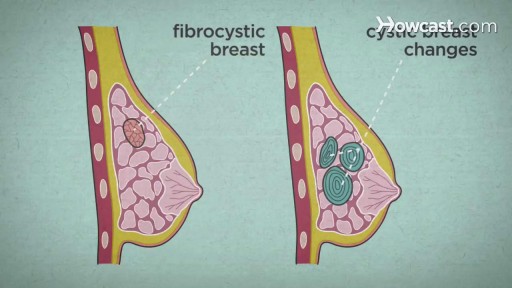
Over the course of a woman's lifetime, she may experience breast changes. While many end up being nothing to worry about, it's important to have any changes that you notice checked by a doctor -- just to be on the safe side. Here are the potential breast cancer symptoms to watch out for.
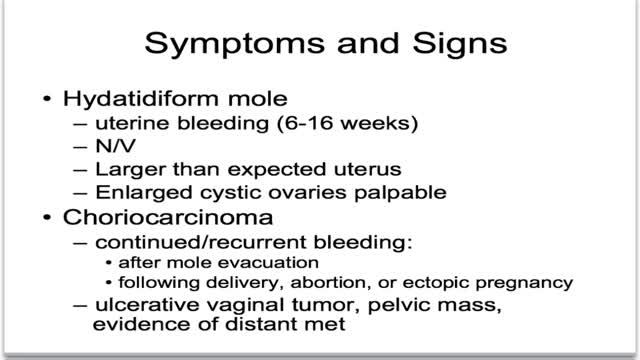
What is gestational trophoblastic disease? Cancer starts when cells in the body begin to grow out of control. Cells in nearly any part of the body can become cancer, and can spread to other areas of the body. To learn more about how cancers start and spread, see What Is Cancer? Gestational trophoblastic (jeh-STAY-shuh-nul troh-fuh-BLAS-tik) disease (GTD) is a group of rare tumors that involve abnormal growth of cells inside a woman's uterus. GTD does not develop from cells of the uterus like cervical cancer or endometrial (uterine lining) cancer do. Instead, these tumors start in the cells that would normally develop into the placenta during pregnancy. (The term gestational refers to pregnancy.) GTD begins in the layer of cells called the trophoblast (troh-fuh-BLAST) that normally surrounds an embryo. (Tropho- means nutrition, and -blast means bud or early developmental cell.) Early in normal development, the cells of the trophoblast form tiny, finger-like projections known as villi. The villi grow into the lining of the uterus. In time, the trophoblast layer develops into the placenta, the organ that protects and nourishes the growing fetus.
Esophageal varices are abnormal, enlarged veins in the tube that connects the throat and stomach (esophagus). This condition occurs most often in people with serious liver diseases. Esophageal varices develop when normal blood flow to the liver is blocked by a clot or scar tissue in the liver. To go around the blockages, blood flows into smaller blood vessels that aren't designed to carry large volumes of blood. The vessels can leak blood or even rupture, causing life-threatening bleeding. A number of drugs and medical procedures can help prevent and stop bleeding from esophageal varices.

Ganglion cysts are noncancerous lumps that most commonly develop along the tendons or joints of your wrists or hands. They also may occur in the ankles and feet. Ganglion cysts are typically round or oval and are filled with a jellylike fluid. Small ganglion cysts can be pea-sized, while larger ones can be around an inch (2.5 centimeters) in diameter. Ganglion cysts can be painful if they press on a nearby nerve. Their location can sometimes interfere with joint movement. If your ganglion cyst is causing you problems, your doctor may suggest trying to drain the cyst with a needle. Removing the cyst surgically also is an option. But if you have no symptoms, no treatment is necessary. In many cases, the cysts go away on their own.
New CPR Guidelines For Adults

This video: Polycystic ovary syndrome (PCOS) is a common endocrine disorder among women of reproductive age. Women with PCOS may have enlarged ovaries that contain small collections of fluid — called follicles — located in each ovary as seen during an ultrasound exam. Infrequent or prolonged menstrual periods, excess hair growth, acne, and obesity can all occur in women with polycystic ovary syndrome. In adolescents, infrequent or absent menstruation may raise suspicion for the condition. The exact cause of polycystic ovary syndrome is unknown. Early diagnosis and treatment along with weight loss may reduce the risk of long-term complications, such as type 2 diabetes and heart disease.
Head CT Interpretation Made Easy
Pruritis is itchy skin that makes you want to scratch. It can be caused by many things. Normally, itchy skin isn't serious, but it can make you uncomfortable. Sometimes, itchy skin is caused by a serious medical condition. It can occur in association with a primary rash (e.g. dermatitis) or may occur because of hypersensitive nerves in the skin (neuropathic pruritus). ... Scratching a localised itch may lead to lichen simplex, prurigo or prurigo nodularis. Systemic causes of pruritus. Sytemic diseases may cause generalised pruritus.
Remove of ascaris lumbricoides worms due to intestinal obstruction

Callus Peel is a luxury, spa foot treatment that removes hard, callused skin leaving your feet feeling soft and revitalised. The treatment is a 15 minute...
An eye web is a noncancerous, triangular growth that may occur on one or both eyes. It's more common in people who spend a lot of time in the sun, such as those who work outdoors. The painless growth may be slightly raised and contain obvious blood vessels. It may cause irritation and possibly affect vision. Treatment usually isn't necessary. Eyedrops or surgery may help in severe cases.

A unique video confirming the reality of the introduction of a large amount of irrigant or drug solution into unoperated paranasal sinuses. How is the process of filling the paranasal sinuses in real time during the YAMIK procedure! The use of the YAMIK Nasal Catheter opens up incredible possibilities for the treatment of sinusitis in both children and adults.

This video: The veins around your anus tend to stretch under pressure and may bulge or swell. Swollen veins (hemorrhoids) can develop from an increase in pressure in the lower rectum. Factors that might cause increased pressure include: Straining during bowel movements.

For education, Microsoft HoloLens will help make incredible leaps forward in productivity, collaboration, and innovation. See how Microsoft HoloLens transforms the way we teach anatomy and our understanding of the human body as we help to prepare the next generation of doctors.
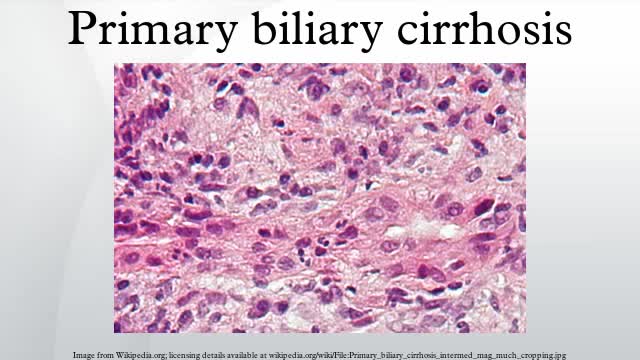
Primary biliary cirrhosis, sometimes called PBC, is a disease in which the bile ducts in your liver are slowly destroyed. Bile, a fluid produced in your liver, plays a role in digesting food and helps rid your body of worn-out red blood cells, cholesterol and toxins. When bile ducts are damaged, as in primary biliary cirrhosis, harmful substances can build up in your liver and sometimes lead to irreversible scarring of liver tissue (cirrhosis). Primary biliary cirrhosis is considered an autoimmune disease, in which the body turns against its own cells. Researchers think it is triggered by a combination of genetic and environmental factors. Primary biliary cirrhosis usually develops slowly and medication can slow its progression, especially if treatment begins early.
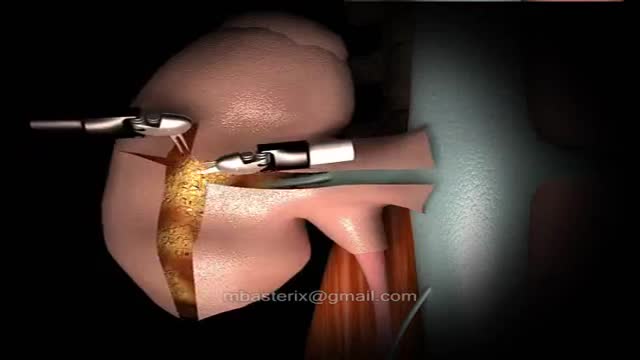
The robotic approach to renal surgery, particularly partial nephrectomy, has some inherent challenges, and some familiarity with the da Vinci robotic system is necessary. The surgeon must gain an understanding of the robotic arm movements and range of motion, especially in relation to the clutch and camera. The advent of robotically assisted prostatectomy in 2001 [23] paved the way for widespread accessibility to the da Vinci robotic unit and its application to renal surgery. Since that time, at least one multi-institutional survey has demonstrated superiority of the robotic approach when compared to laparoscopic for outcomes of blood loss, hospital stay and a substantially shorter warm ischemia time, while maintaining equivalence in positive margin rate, operative time and complications. [11] A transperitoneal approach is most commonly used. Prior abdominal operation is not necessarily a contraindication to this procedure, but access should be approached with regard for previous operation(s) by an experienced team.
Failing Kidneys and Different Treatment Options
We present a cases of child of age 4 yrs with open safety pin (SP) impacted in the U/3 esophagus and description of the techniques used for their removal
Check out how Physician Coder – an online specialty solution – can help you meet your practice’s goals for error-free coding. From helping you meet all your ICD-10 coding needs from one place with code lookup, crosswalk, superbill converter, scrubber, and monthly specialty articles to helping you review CPT® 2016 changes with expert analysis for your specialty, we have you covered. Plus, you’ll also learn how to stay up-to-date on 2016 fee schedule details like RVUs, global days, and MUEs; check the latest CCI edits and view LCD policy details.
