- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

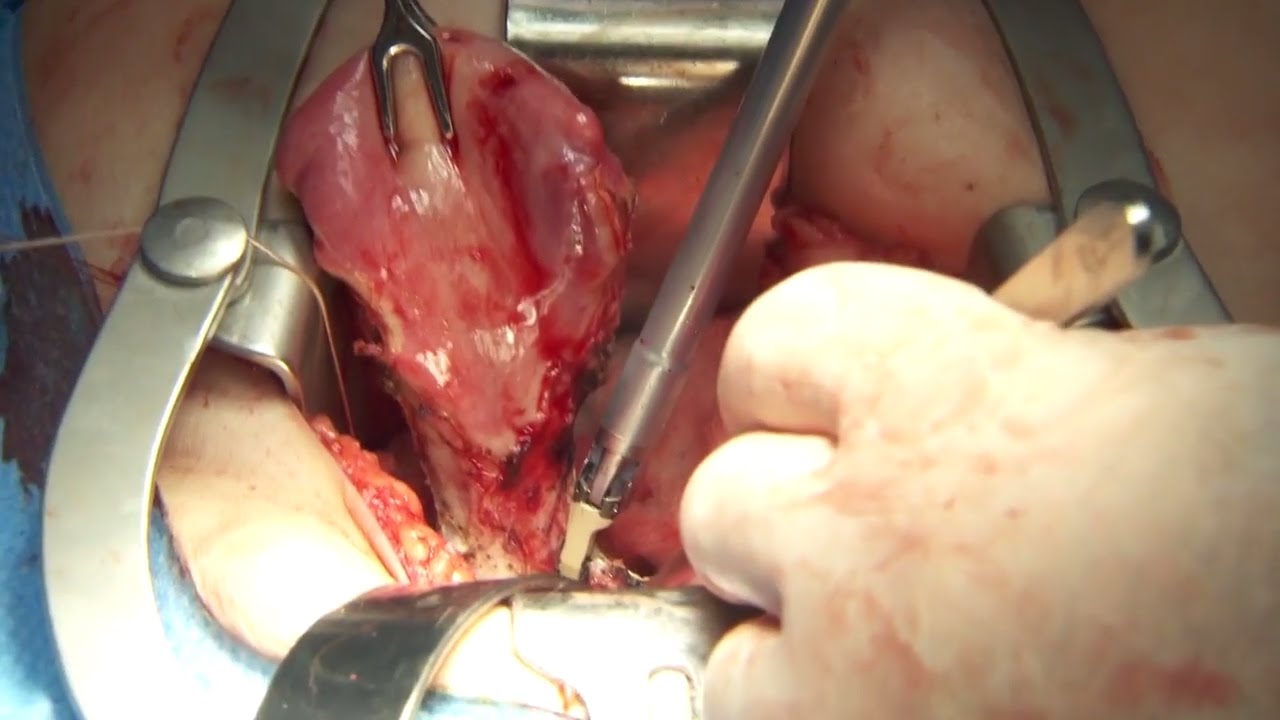
Perineal Protectomy for Rectal Prolapse

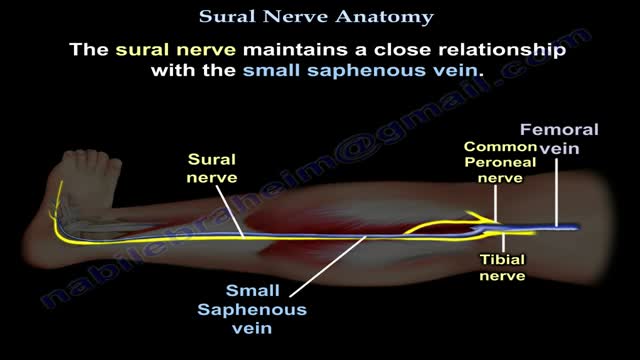
Nerves are the organs that make up the peripheral nervous system (PNS). They serve as information pipelines that allow the brain and spinal cord to communicate with other tissues and organs. Inside the nerves are the axon processes of sensory and motor neurons (nerve cells).
The video will describe what is sarcoidosis. Please see my website for disclaimer.
the video will describe oxyhemoglobin dissociation curve. please see my website for disclaimer.

Watch that video to know What is Vaginal Discharge and How To Get Rid of It
Coronary artery bypass grafting (CABG) is a type of surgery that improves blood flow to the heart. Surgeons use CABG to treat people who have severe coronary heart disease (CHD). CHD is a disease in which a waxy substance called plaque (plak) builds up inside the coronary arteries.
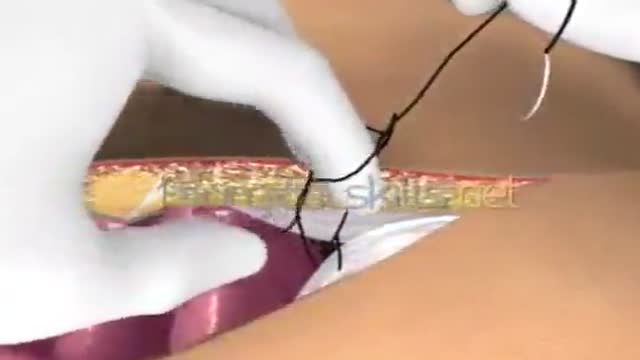
Laparotomy Closure Abdomen Animation

Volar Slab Splint for Forearm and Wrist Fractures and Sprains
Abdominal aortic aneurysms can weaken the aorta, your body’s largest blood vessel. This can develop into a potentially serious heath problem that can be fatal if the aneurysm bursts, causing massive internal bleeding. Endovascular stent grafting, or endovascular aneurysm repair (EVAR), is a newer form of treatment for abdominal aortic aneurysm that is less invasive than open surgery. Endovascular stent grafting uses an endovascular stent graft to reinforce the wall of the aorta and to help keep the damaged area from rupturing.
Watch that video to know How To Increase Testosterone Levels Naturally

Watch that Cutting Inside Human Fat Body video
Olympus has extended the value of its award-winning combined surgical energy device, THUNDERBEAT, to open surgical procedures. Watch Dr. Francois Blaudeau master use of THUNDERBEAT Open Extended Jaw (OEJ) in a total abdominal hysterectomy.
http://medical.olympusamerica.com/products/thunderbeat?utm_source=youtube&utm_campaign=Total%20Abdominal%20Hysterectomy%20Surgery%20-%20THUNDERBEAT&utm_medium=description&utm_term=energy&utm_content=surgical
Extradural approach via Orbito-Zygomatic Craniotomy

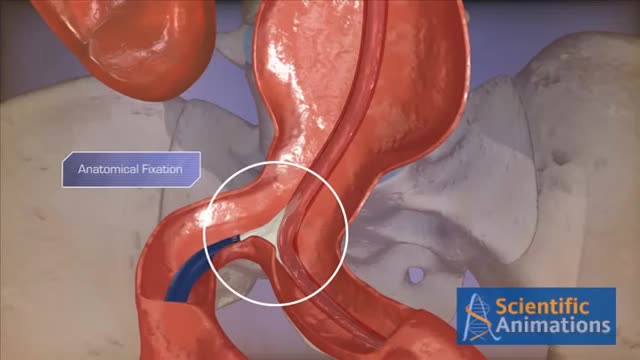
Do you think you have a hernia?
What are hernias?
The hernias we address in this http://DoctorsExpressHartsdale.com Medical Minute are inguinal, or groin, hernias. More common in men than women, an inguinal hernia can occur when part of the small intestine protrudes through a weakness or tear in the area between your abdomen and your thigh- or your groin. It's possible for anyone to get an inguinal hernia, but it is more commonly found in males.
Hernias form a bulge and can be accompanied by pain. Men have an approximate 26% lifetime risk of having hernia at some point in their life, where as women have a much lower chance of one- only about 3% of women will experience a hernia at some point in their life. There are other types of hernias, such as abdominal, or "hiatal" hernias but groin hernias outnumber abdominal hernias by about 3 to 1.
What causes a hernia?
The cause of a hernia is not always known, but hernias are often the result of weak spots in the abdominal wall. Weaknesses can be due to congenital defects (present at birth) or formed later in life. Some risk factors for inguinal hernia include:
• fluid or pressure in the abdomen
• heavy lifting
• straining during urination or bowel movements
• obesity
• chronic cough
• pregnancy
Hernias often form in people with weakened abdominal muscles or in those who do a lot of heavy lifting or straining, which is why we see it quite often in young men. Physiology plays a part: men have testicles and scrotum which descend through the inguinal canal-much larger in men than in women. That is part of the reason men tend to be more susceptible to hernias than women.
Symptoms of hernia
Symptoms of inguinal hernia usually include a bulge in the groin area and pain, pressure, or aching at the bulge—especially when lifting, bending, or coughing. These symptoms usually subside during rest periods. Men may also experience swelling around the testicles.
Screening and Diagnosis of Hernias
If you are having abdominal pain or pelvic bulge and pain, you want to see physician, and he or she will do an exam. They will use their finger, to see if you have a bulge in your scrotum or on your groin and they'll see if its reducible or not. If the exam doesn't give them the answer, they can then perform an ultrasound, an inexpensive test that can tell you the same day whether a hernia is present.
What to do if you think you have a hernia
Most of the time hernias do not cause problems. People often live with hernias their entire life without them becoming aggravated or painful. When they do cause pain though, there is concern that complications may have arisen. Most common hernias are what we call reducible; you can take your finger or you can lie down in bed and due to the effects of gravity, the bulge in the groin will actually disappear, which means the intestinal contents actually go back into the abdominal cavity or to the correct location. If it's not reducible by lying down or using a finger or having a physician trying to reduce it, then there are concerns about complications such as strangulation, or incarceration occurring. If those concerns are there, then you need to see a surgeon, and there may be a need for surgery.
How to Treat a Hernia
As stated earlier, hernias can often be watched for years without being treated. If however, they are causing pain, we generally refer you to a surgeon who can do a very simple laparoscopic surgery.
If you suspect a hernia, but have not been diagnosed, you should see your doctor, and of course, we are happy to see you here at Doctors Express

Rehydration Tips: Kids & Teens (Ages 1+) Give clear liquids (avoid milk and milk products) in small amounts every 15 minutes. ... If your child vomits, start over with a smaller amount of fluid (2 teaspoons, or about 10 milliliters) and continue as above. ... After no vomiting for about 8 hours, introduce solid foods slowly.

Asthma Mechanism 3D

A new procedure helps patients with unattractive bunions and hammertoes.
Glaucoma Surgery 3D Animation

It may be reassuring to know spotting or bleeding after sex is common and can come from the vagina, cervix, or urinary tract. It occurs most commonly in women 20 to 40 years old. Cervical Cancer: A very rare cause of spotting. ... Vaginal Dryness: Often caused by inadequate foreplay or vaginal lubrication.
