Toppvideor

breast self examination
Arachnoid Cyst Brain Surgery HD
Anatomy of The Pharynx

Anatomy of The Infratemporal Fossa
The first step is to see if you have pigmentation issues -not really classed as acne scars, but this is controversial, or if you have contour changes. The best thing to do is to examine under tangential or angled lighting, as this will reveal all. Once this is done, scars can be subtyped and mapped, with high resolution photos. The second aspect, which is equally as important is to examine scars upon animanation, namely when you speak, smile and move your face. This will give me an idea of the amount of tethering and anchored acne scars. Time and time again I get request for ‘what is the treatment’ with static photos, an impossible task to answer correctly. Acne scar assessment has to be done live- with the patient in front of you, and lighting from all angles. Photos do not map scars as well a real time examination under magnification and lighting.

What is this white substance coming out from my skin pores everytime I squeeze my nose or chin?
Plastic Surgery Disasters
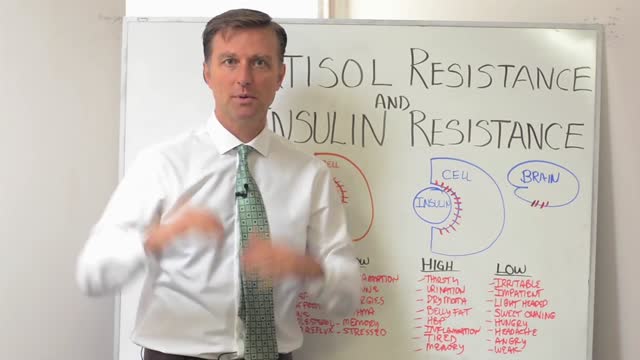
Insulin resistance — also called syndrome X or metabolic syndrome— is so pervasive today that we evaluate nearly every woman who visits our clinic to determine her level of risk. Most are taken aback when they learn they either already have insulin resistance syndrome (or as I call it pre-pre diabetic) or are well on their way to developing it. Experts estimate that 25% of all Americans suffer from insulin resistance. We believe the percentage is much higher among perimenopausal women. Because insulin is one of the “major” hormones, it’s also impossible for your body to balance its “minor” hormones (estrogen, progesterone and testosterone among them) until your insulin metabolism is balanced first. To put it simply, if you have hot flashes and you are insulin resistant, it’s going to be nearly impossible to cure the hot flashes without first healing the insulin resistance. Cortisol is also a “major” hormone – to understand it’s role in hormonal balance, read our related articles on adrenal fatigue. The good news is that you can heal insulin resistance. This has been a primary focus of our practice at Women to Women for over a decade, and our approach has been quite successful. Throughout the website you will find simple solutions on how to begin to heal this problematic syndrome.
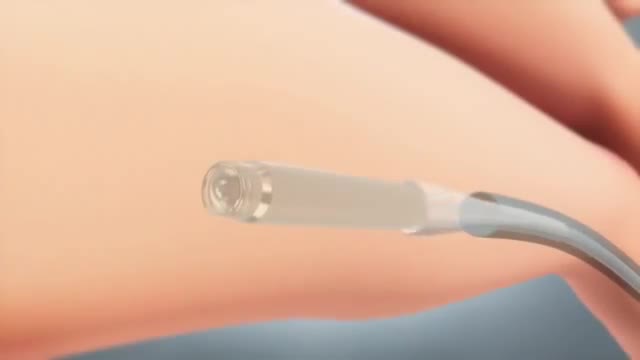
This tiny wireless pacemaker can be inserted into the body via a catheter instead of invasive surgery.
Uncontrolled hyperthyroidism during pregnancy can lead to serious health problems in the mother and the unborn baby. During pregnancy, mild hyperthyroidism does not require treatment. More severe hyperthyroidism is treated with antithyroid medications, which act by interfering with thyroid hormone production.

Stomach acid is natural, a valuable chemical contributor to orderly digestion. But in excess or in the wrong place, it's a menace, inflaming and irritating the esophagus, typically causing heartburn and sometimes contributing to the development of ulcers in the stomach and the duodenum, the first part of the small intestine.
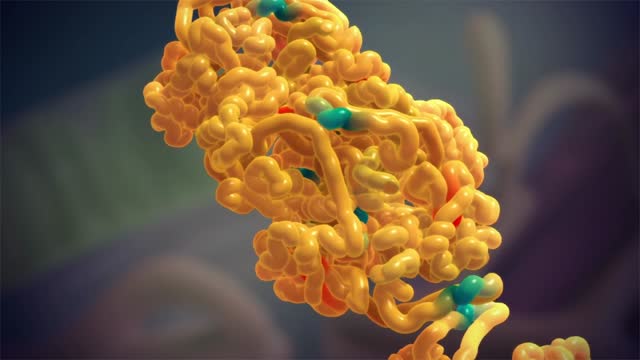
Amyloidosis (am-uh-loi-DO-sis) is a rare disease that occurs when a substance called amyloid builds up in your organs. Amyloid is an abnormal protein that is usually produced in your bone marrow and can be deposited in any tissue or organ. Amyloidosis can affect different organs in different people, and there are different types of amyloid. Amyloidosis frequently affects the heart, kidneys, liver, spleen, nervous system and digestive tract. Severe amyloidosis can lead to life-threatening organ failure.
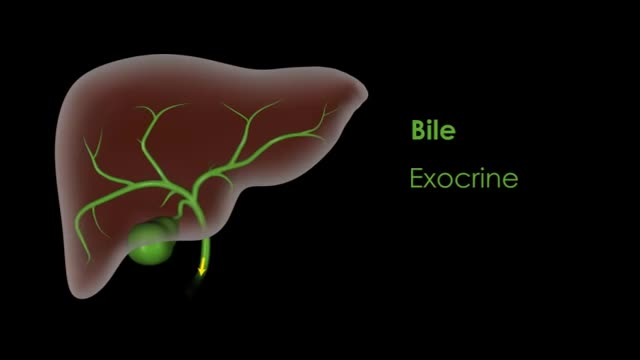
liver also detoxifies chemicals and metabolizes drugs. As it does so, the liver secretes bile that ends up back in the intestines. The liver also makes proteins important for blood clotting and other functions.
The cell membrane is selectively permeable to ions and organic molecules and controls the movement of substances in and out of cells. The basic function of the cell membrane is to protect the cell from its surroundings. It consists of the phospholipid bilayer with embedded proteins.
On the day of your surgery, your health care team will take you to a preparation room. Your blood pressure and breathing will be monitored. You may receive an antibiotic medication through a vein in your arm. You will then be taken to an operating room and positioned on a table. You'll be given a general anesthesia medication to put you in a sleep-like state so that you won't be aware during your operation. The surgical team will then proceed with your colectomy. Colon surgery may be performed in two ways: Open colectomy. Open surgery involves making a longer incision in your abdomen to access your colon. Your surgeon uses surgical tools to free your colon from the surrounding tissue and cuts out either a portion of the colon or the entire colon. Laparoscopic colectomy. Laparoscopic colectomy, also called minimally invasive colectomy, involves several small incisions in your abdomen. Your surgeon passes a tiny video camera through one incision and special surgical tools through the other incisions. The surgeon watches a video screen in the operating room as the tools are used to free the colon from the surrounding tissue. The colon is then brought out through a small incision in your abdomen. This allows the surgeon to operate on the colon outside of your body. Once repairs are made to the colon, the surgeon reinserts the colon through the incision. The type of operation you undergo depends on your situation and your surgeon's expertise. Laparoscopic colectomy may reduce the pain and recovery time after surgery. But not everyone is a candidate for this procedure. Also, in some situations your operation may begin as a laparoscopic colectomy, but circumstances may force your surgical team to convert to an open colectomy. Once the colon has been repaired or removed, your surgeon will reconnect your digestive system to allow your body to expel waste. Options may include: Rejoining the remaining portions of your colon. The surgeon may stitch the remaining portions of your colon together, creating what is called an anastomosis. Stool then leaves your body as before. Connecting your intestine to an opening created in your abdomen. The surgeon may attach your colon (colostomy) or small intestine (ileostomy) to an opening created in your abdomen. This allows waste to leave your body through the opening (stoma). You may wear a bag on the outside of the stoma to collect stool. This can be permanent or temporary. Connecting your small intestine to your anus. After removing both the colon and the rectum (proctocolectomy), the surgeon may use a portion of your small intestine to create a pouch that is attached to your anus (ileoanal anastomosis). This allows you to expel waste normally, though you may have several watery bowel movements each day. As part of this procedure, you may undergo a temporary ileostomy.

Endoscopic retrograde cholangiopancreatography, or ERCP, is a specialized technique used to study the bile ducts, pancreatic duct and gallbladder. Ducts are drainage routes; the drainage channels from the liver are called bile or biliary ducts. The pancreatic duct is the drainage channel from the pancreas.

Medical Terminology
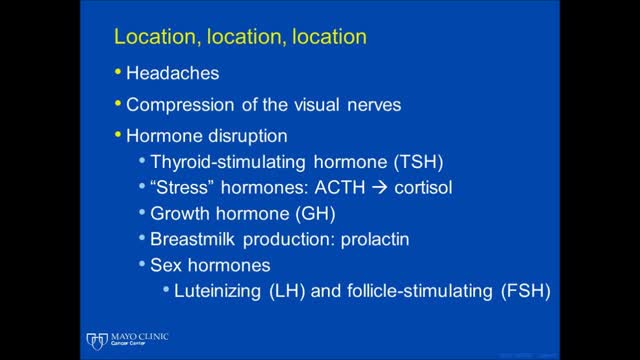
Multiple endocrine neoplasia is a group of disorders that affect the body's network of hormone-producing glands (the endocrine system). Hormones are chemical messengers that travel through the bloodstream and regulate the function of cells and tissues throughout the body. Multiple endocrine neoplasia typically involves tumors (neoplasia) in at least two endocrine glands; tumors can also develop in other organs and tissues. These growths can be noncancerous (benign) or cancerous (malignant). If the tumors become cancerous, the condition can be life-threatening.

Euthyroid sick syndrome (ESS), sick euthyroid syndrome (SES), thyroid allostasis in critical illness, tumours, uremia and starvation (TACITUS), non-thyroidal illness syndrome (NTIS) or low T3 low T4 syndrome is a state of adaptation or dysregulation of thyrotropic feedback control where the levels of T3 and/or T4 are ...
Toxoplasmosis (tok-so-plaz-MOE-sis) is a disease that results from infection with the Toxoplasma gondii parasite, one of the world's most common parasites. Toxoplasmosis may cause flu-like symptoms in some people, but most people affected never develop signs and symptoms. For infants born to infected mothers and for people with weakened immune systems, toxoplasmosis can cause extremely serious complications. If you're generally healthy, you probably won't need any treatment for toxoplasmosis. If you are pregnant or have lowered immunity, certain medications can help reduce the infection's severity. The best approach, though, is prevention.
