- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
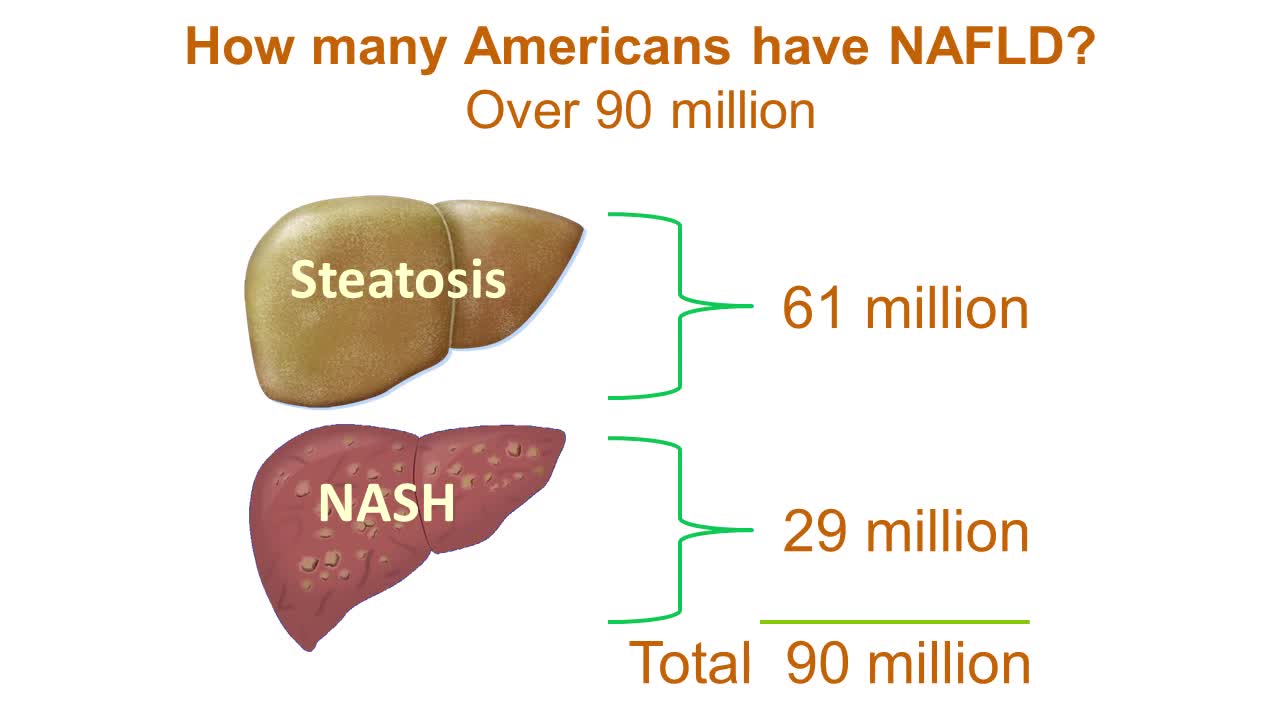
Nonalcoholic fatty liver disease is an umbrella term for a range of liver conditions affecting people who drink little to no alcohol. As the name implies, the main characteristic of nonalcoholic fatty liver disease is too much fat stored in liver cells. Nonalcoholic steatohepatitis, a potentially serious form of the disease, is marked by liver inflammation, which may progress to scarring and irreversible damage. This damage is similar to the damage caused by heavy alcohol use. At its most severe, nonalcoholic steatohepatitis can progress to cirrhosis and liver failure Nonalcoholic fatty liver disease is increasingly common around the world, especially in Western nations. In the United States, it is the most common form of chronic liver disease, affecting an estimated 80 to 100 million people. Nonalcoholic fatty liver disease occurs in every age group but especially in people in their 40s and 50s who are at high risk of heart disease because of such risk factors as obesity and type 2 diabetes. The condition is also closely linked to metabolic syndrome, which is a cluster of abnormalities including increased abdominal fat, poor ability to use the hormone insulin, high blood pressure and high blood levels of triglycerides, a type of fat. Nonalcoholic fatty liver disease care at Mayo Clinic Request an Appointment at Mayo Clinic Symptoms & causes Aug. 23, 2016 Print Share on: Facebook Twitter References Related Magnetic resonance elastography Nonalcoholic fatty liver disease Overview Symptoms & causes Diagnosis & treatment Diagnosis Treatment Departments & specialties Expertise & rankings Locations, travel & lodging Clinical trials Research Costs & insurance Preparing for your appointment Self-management More about In-Depth Multimedia Resources News from Mayo Clinic Advertisement

Baby Born Still Inside The Amniotic Sac
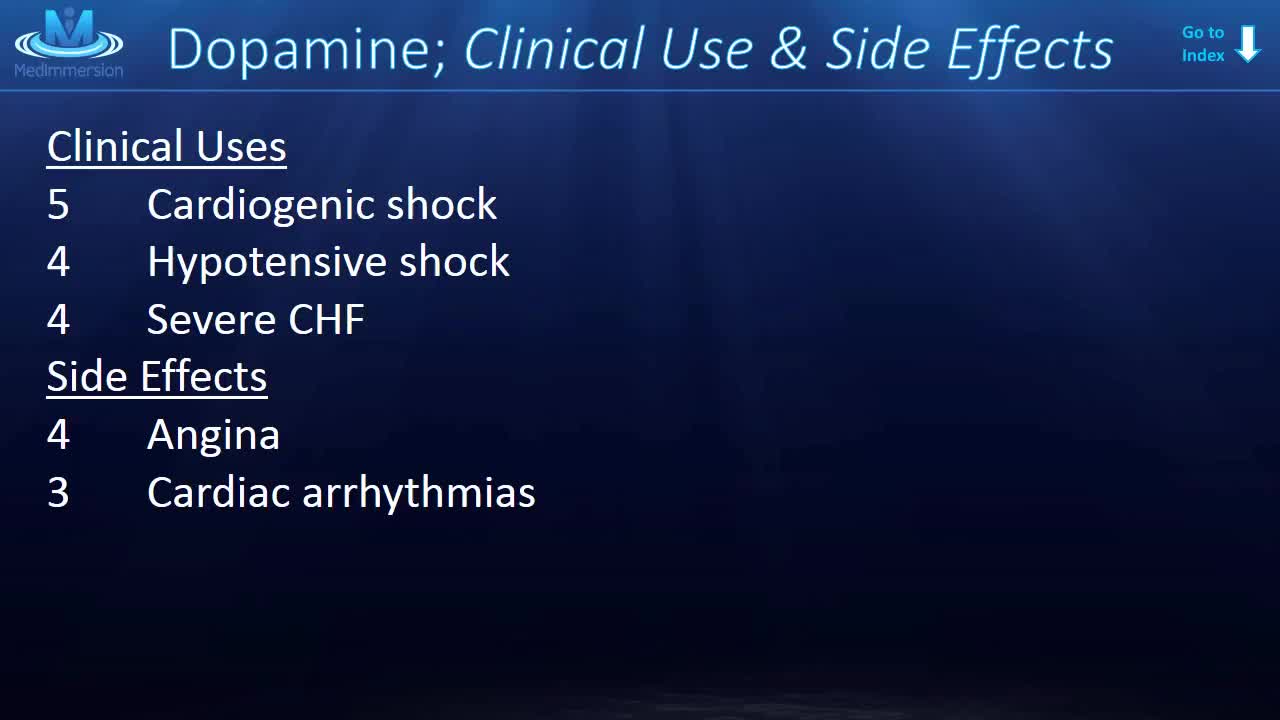
Dopamine is the one neurotransmitter that everyone seems to know about. Vaughn Bell once called it the Kim Kardashian of molecules, but I don’t think that’s fair to dopamine. Suffice it to say, dopamine’s big. And every week or so, you’ll see a new article come out all about dopamine.

in this patient the aneurysm wasarising from middle cerebral artery M1 segment dividng into three branches,it is mandatory topreserve all three divisions,as was done in this case,this pt 25 yrs young man presented with sub arachnoid haemorrhage
www.lung.org > Lung Health and Diseases > Lung Disease Lookup > Silicosis Learn About Silicosis Silicosis is a lung disease caused by breathing in tiny bits of silica, a mineral that is part of sand, rock, and mineral ores such as quartz. It mostly affects workers exposed to silica dust in occupations such mining, glass manufacturing, and foundry work. Over time, exposure to silica particles causes scarring in the lungs, which can harm your ability to breathe. Key Facts There are three types of silicosis: acute, chronic, and accelerated. It occurs in workers from mines, foundries, sandblasting, and glass manufacturing. About 2 million US workers remain potentially exposed to occupational silica. There is no cure for silicosis, but it can be prevented. What Is Silicosis? There are three types of silicosis: Acute silicosis, which causes cough, weight loss, and fatigue within a few weeks or years of exposure to inhaled silica. Chronic silicosis, which appears 10 to 30 years after exposure and can affect upper lungs and sometimes cause extensive scarring. Accelerated silicosis, which occurs within 10 years of high-level exposure. Silicosis can develop within a few weeks to even decades after exposure. When people breathe silica dust, they inhale tiny particles of the mineral silica. This silica dust can cause fluid buildup and scar tissue in the lungs that cuts down your ability to breathe. This can lead to lung scarring and cough, weight loss, and fatigue.

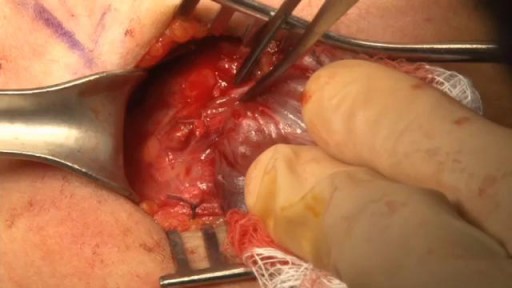
This video shows doctors removing two long ascaris worms from liver.

Woman suffers allergic reaction to nut protein in boyfriend's sperm.A British woman has become the first recorded case of someone suffering an allergic...

New-born baby having a bath

why you should keep your ears clean.
Watch that video to know How To Increase Testosterone Levels Naturally

http://combatir-la-ansiedad.good-info.co/ --- Como Calmar La Ansiedad, Ataque De Ansiedad Que Hacer, Remedios Naturales Para La Ansiedad. Como ir curando tu ansiedad... ¿De seguro te sientes desesperado por no poder saber como poder curar tu ansiedad cierto? No te preocupes, esto se puede solucionar. Muchas veces probamos todo tipo de tratamientos que al final muchas veces hace que todo se haga mucho mas dificil. Tanto que inclusive al final sentimos que hemos empeorado todo ¿cierto? Sin la guia adecuada, parece como si nunca fueras encontrar el metodo correcto para poder vivir una vida libre de ansiedad. Afortunadamente actualmente existe una guia la cual te ahorrara el camino dificil y asi podras ir eliminando todos esos sintomas que te hace sentir miedo y ansiedad. para que asi puedas vivir una vida en paz y llena de alegria. Si quieres conocer más tan solo visita este enlace. http://combatir-la-ansiedad.good-info.co
Chicken Skin, Chicken Skin On Legs, Keratosis Pilaris Treatment Over The Counter, Kp Vitamin A--- http://banishmybumps.plus101.com/ --- What Causes KP? The particular cause of Keratosis Pilaris is unidentified. Usually, it happens when there is a difficulty on the production of the keratin that is called hyper keratinizatinization. Keratosis Pilaris is believed to be inherited partially in origin. About fifty percent up to seventy percent of patients with this type of skin condition have identified genetic predisposition and has a higher rate of affected members of the family. Most people have a solid family history of follicular pilaris. The primary cause may be related partly to hypersensitivity reactions as well as the overall skin dryness. This skin condition is closely related also to dry skin, allergies, asthma, eczema, atopic dermatitis and rhinitis. The red bumps in Keratosis Pilaris seem to rise from the unnecessary build-up of keratin dry skin particles and very small at the hair follicles opening. The skin as observed under the hand held microscope demonstrates mild condensing, plugging and hyperkeratosis of your hair follicle. Your upper skin layers may have a number of dilation of the minor superficial blood vessels. In this manner, it gives the skin a flushed or reddish appearance. Keratosis Pilaris is not infectious, therefore people surrounding you are safe from this irritating skin condition. The condition is worse during winter. Summer season is normally a reprieve as it brings moisture and usually allows the skin condition to smooth up more than normal. The aggravating is associated directly with lower moisture, tight clothes and skin dryness that cause to rub the red bumps all the times. Many people stated that this skin condition worsened during the period of pregnancy before and after child birth. Medical doctors and patients as well, believed that keratosis pilaris is also related to food intake. So, large intakes of spicy foods increase the form of red bumps that make them more visible. In some way, patients that eliminated or reduced milk as well as the derivatives from their balance diet stated the improvement of their condition. Keratosis Pilaris can be difficult to treat, but it is possible to seek permanent relief. New research shows that all-natural treatment systems, such as BanishMyBumps, are successful. You can learn more at http://banishmybumps.plus101.com/
Colon Irritable Tratamiento Natural, Tratamiento Sindrome Intestino Irritable, Colon Irritable Cura--- http://intestino-irritable-tratamiento.plus101.com --- Los Alimentos Desencadenantes De SCI, Esta dolencia gastrointestinal puede ser desencadenada por ciertos alimentos o grupos de alimentos, de los cuales podemos mencionar específicamente seis de ellos. Lo aconsejable es que evite su consumo si usted sufre o es propenso a sufrir SII. 1 - Los alimentos fritos, especialmente los fritos con aceites que contienen ácidos grasos trans hidrogenados. Dentro de este grupo encontramos las llamadas comidas rápidas. 2 - La carne y los productos lácteos: las carnes grasas, especialmente de las granjas industriales, carnes procesadas y la leche pasteurizada. Para reemplazar estos alimentos, se puede utilizar leche de soja o la llamada carne orgánica, proveniente de ganado alimentado a base de pasto, libre de químicos, antibióticos y hormonas de crecimiento. 3 - Los productos horneados procesados incluyendo panes envasados, pasteles y galletas. Contienen azúcar refinada y grasas malas, así como harina blanca refinada. A veces es posible que contengan jarabe de maíz alto en fructosa. Si usted sufre del SII, puede optar por la compra de productos de panadería directamente de una panadería de su confianza o hacer sus propios productos caseros con ingredientes enteros. Trigo germinado, los sustitutos del trigo, como el trigo sarraceno espelta, u otros granos utilizados en productos de panadería (sin aditivos perjudiciales) también pueden ser una opción que no va a afectar a su organismo. Lea atentamente las etiquetas de los productos que consume y ante cualquier duda, debe asesorarse. 4 - El café y el alcohol pueden crear respuestas ácidas del esfínter inferior del esófago y la válvula ileocecal, que es el esfínter entre los intestinos grueso y delgado que se abre brevemente y se cierre la mayor parte del tiempo para evitar que los fluidos intestinales se mezclen. La causa principal de muchos de los problemas del SII y de otras enfermedades digestivas más graves se da cuando la válvula ileocecal permanece abierta demasiado tiempo. Todas las demás recomendaciones relativas a los alimentos y los hábitos alimentarios son relevantes para evitar que esto ocurra. 5 - Los edulcorantes artificiales: El sorbitol puede no ser tan peligroso neurológicamente como el aspartamo y otros edulcorantes artificiales, pero estimula los síntomas del SII. Para obtener más consejos sobre alimentación sana que lo ayude a aliviar sus síntomas del SII, puede dirigirse al sitio http://intestino-irritable-tratamiento.plus101.com
Watch that Thyroid Removal Surgery
Natural Ways To Stop Hair Loss, Hair Regrowth Home Remedies, Best Medicine For Hair Regrowth---- http://how-to-regrow-your-hair.info-pro.co/ --- What Is The Best Male Hair Loss Treatment? Well there are actually many that can be given. The reason for this is simple – male hair loss is not caused by a singular problem alone. Hair loss can be caused by genetics, stress, aging, and others and thus the treatment will be different for each one. If you are talking about hair loss related to genetics however then there are a few products or procedures that you might want to take note of. Pattern hair loss or Male pattern hair loss is called Androgenic Alopecia. It’s basically the result of hormones called androgens which is caused by genetic predisposition. To put it simply, the reason you are losing your hair is because you are genetically predisposed to. The general rule of thumb is that hair can still be thickened anywhere that it’s still growing and a hair loss treatment regimen is one of the most effective solutions you have at hand. An area that is already slick and hairless will most likely not impossible to restore, and hair transplants or a hair system is your best bet for this. Since many combinations of thinning and slick are often present in men, a treatment regimen is most often the best or sometimes the only solution available. Transplants and hair systems or toupees should only be considered if you have already undergone a treatment regiment for two solid years without achieving any satisfactory results. No matter the type or situation you are dealing with, a scientifically backed hair loss treatment regimen is necessary. Learn the science behind HOW you can Re-Grow your hair and discover the logical solution to eliminate your balding....effectively, naturally and permanently http://how-to-regrow-your-hair.info-pro.co/

tretment
kids react to games

Removal of drain tube after spleen surgery
15th August Special Offer - Get 50% discount on Chemical Peel & Medical Facial ! offer valid till 31st August 2018 ! Call now 09958221983 to book appointment! Send your Query: info@drkashyap.com #MedicalFacial #ChemicalPeels #Facial #SkinCare #NonSurgical #Treatments #Clinic #Delhi #India #15thAugust #IndependenceDay

Laparoscopic use of Palmer's Point
