Top Videos


A video showing the PRK laser eye surgery

Endoscopic Brain Surgery, third Ventriculostomy

different aging and other skin spots can be treated succesfully with Co2 laser.
This is an amazing device designed to transport body organs and blood long distances. The inventor of this life-saving device is Randal Miller.

Laser Liposuction for Weight Loss
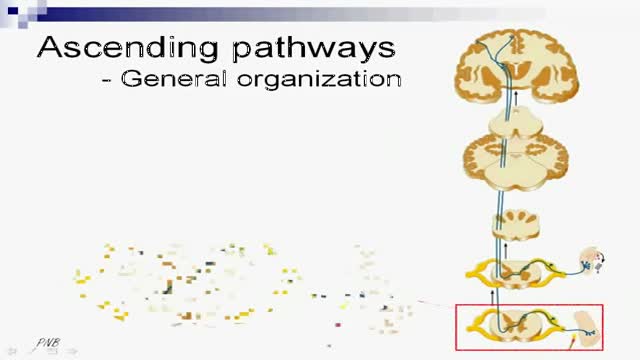
A tutorial showing ascending sensory pathways
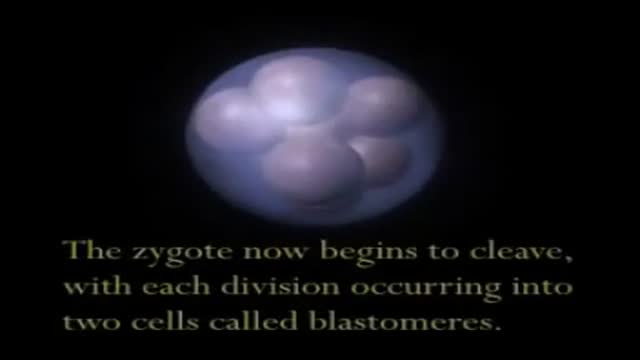
A video showing Embryo and Fetal Development

Carpal Tunnel Syndrom 3D Animation
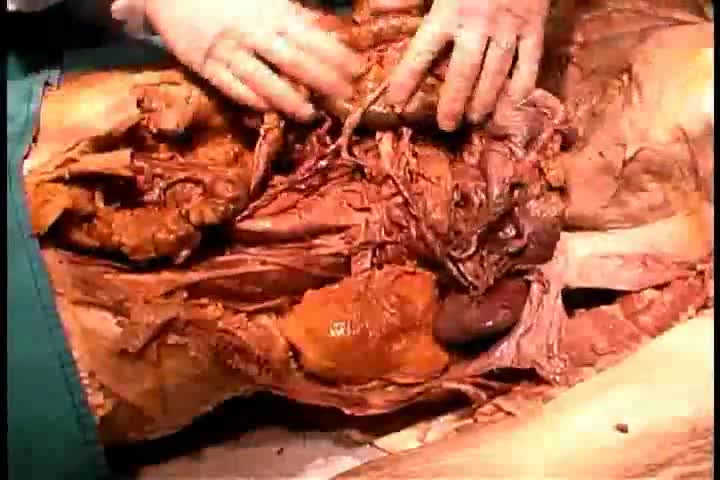
Anatomy of The Abdominal Autonomic Nerve Supply

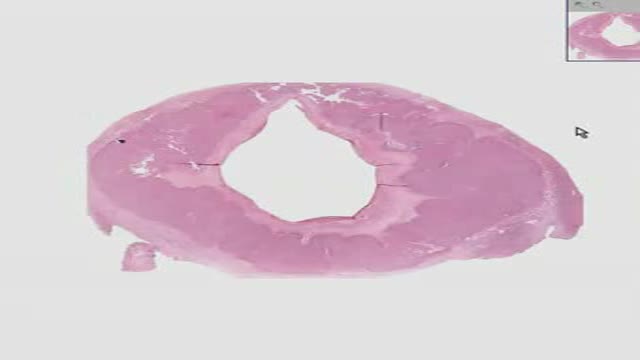
Histology of GastroEsophageal Junction
Histology of Corpus Luteum 1

Dextrocardia situs inversus refers to the heart being a mirror image situated on the right side. For all visceral organs to be mirrored, the correct term is dextrocardia situs inversus totalis. Dextrocardia is believed to occur in approximately 1 in 12,000 people.

Fake Sonogram

If you are self-conscious because you have missing teeth, wear dentures that are uncomfortable or don't want to have good tooth structure removed to make a bridge, talk to your dentist to see if dental implants are an option for you. Dental implants are a popular and effective way to replace missing teeth and are designed to blend in with your other teeth. They are an excellent long-term option for restoring your smile. In fact, the development and use of implants is one of the biggest advances in dentistry in the past 40 years. Dental implants are made up of titanium and other materials that are compatible with the human body. They are posts that are surgically placed in the upper or lower jaw, where they function as a sturdy anchor for replacement teeth.
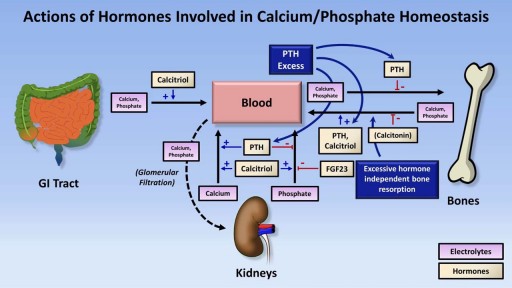
Alendronate Sodium is used for the following diseases and conditions: osteoporosis, and osteogenesis imperfecta. Alendronate Sodium improves the patient's condition by performing the following functions: slowing down the bone loss and helps to keep the bones strong and less likely to break. Side effects are possible with Alendronate Sodium, but do not always occur. Some of the side effects may be rare but serious. Consult your doctor if you observe any side effects, especially if they do not go away. Alendronate Sodium may cause the following side-effects: stomach pain, constipation, diarrhea, gas, nausea, and jaw pain
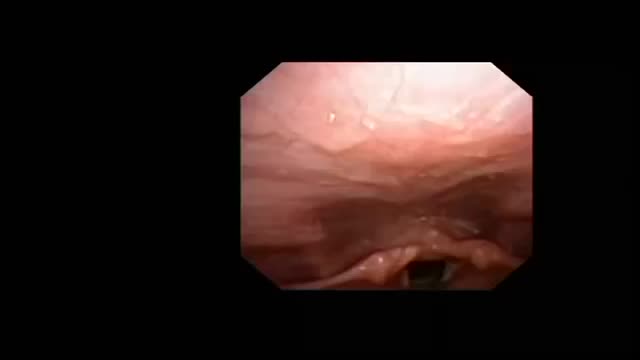
High Resolution Upper Airway Anatomy

Experts do not know the exact cause of Zollinger-Ellison syndrome. About 25 to 30 percent of gastrinomas are caused by an inherited genetic disorder called multiple endocrine neoplasia type 1 (MEN1). MEN1 causes hormone-releasing tumors in the endocrine glands and the duodenum.

blood transfusion performance
