- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
What is heparin injection? Heparin is an anticoagulant (blood thinner) that prevents the formation of blood clots. Heparin is used to treat and prevent blood clots in the veins, arteries, or lung. It is also used before surgery to reduce the risk of blood clots. Heparin works by inactivating thrombin in the clotting process. This stops the formation of fibrin and so stops blood clots forming. Heparin is used to treat blood clots that have formed abnormally inside the blood vessels. It can also be used to prevent these types of dangerous blood clots.
Your body is a brilliant machine with many important parts. Watch movies to learn more
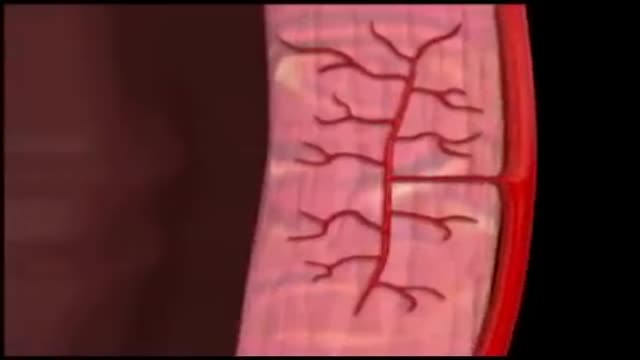
Coronary circulation is the circulation of blood in the blood vessels of the heart muscle (myocardium). The vessels that deliver oxygen-rich blood to the myocardium are known as coronary arteries. The vessels that remove the deoxygenated blood from the heart muscle are known as cardiac veins.
Gastroparesis is a disorder affecting people with both type 1 and type 2 diabetes in which the stomach takes too long to empty its contents (delayed gastric emptying). The vagus nerve controls the movement of food through the digestive tract. If the vagus nerve is damaged or stops working, the muscles of the stomach and intestines do not work normally, and the movement of food is slowed or stopped. Just as with other types of neuropathy, diabetes can damage the vagus nerve if blood glucose levels remain high over a long period of time. High blood glucose causes chemical changes in nerves and damages the blood vessels that carry oxygen and nutrients to the nerves. - See more at: http://www.diabetes.org/living-with-diabetes/complications/gastroparesis.html?referrer=https://www.google.com/#sthash.rTgZiOuM.dpuf

Blood type (or blood group) is determined, in part, by the ABO blood group antigens present on red blood cells. A blood type (also called a blood group) is a classification of blood based on the presence or absence of inherited antigenic substances on the surface of red blood cells (RBCs).

A ventricular septal defect (VSD) is an opening or hole in the wall that separates the two lower chambers of the heart. This wall is called the ventricular septum. The hole causes oxygen-rich blood to leak from the left side of the heart to the right side. This causes extra work for the right side of the heart, since more blood than necessary is flowing through the right ventricle to the lungs. The hole is usually closed with surgery. However, in certain situations, your child's cardiologist and surgeon may think it is best to close the hole with a special device. This procedure is done in the heart catheterization lab.

The pain of ovulation can range from a mild twinge to severe discomfort and usually lasts from minutes to hours. It is generally felt on one side of the abdomen and may vary each month, depending on which ovary is releasing the egg during that cycle.

It's a symptom of heart disease but typically does not cause permanent damage to the heart. It is, though, a sign that you are a candidate for a heart attack at some point in the future. The chest pain may spread to your arm, shoulder, jaw, or back. It may feel like a pressure or squeezing sensation.

Your doctor says your chest pain (angina) is caused by blockages in your heart arteries and that you need to get those blockages taken care of. What are your options? First, it's important to determine what type of angina you have. Different types of angina may need different treatments. Common types of angina are chronic stable angina — a type of angina that occurs when your heart is working hard — and unstable angina, which is new chest pain or chest pain that is getting worse. Other types of angina include variant angina — a rare type of angina caused by a spasm in the coronary arteries — and microvascular angina, which can be a symptom of disease in the small coronary artery blood vessels. Unstable angina is a serious situation and requires emergency treatment. Treatment for unstable angina involves hospitalization with medications to stabilize your condition. Some people with unstable angina may require a procedure called angioplasty (also known as percutaneous coronary intervention), usually combined with the placement of a small metal tube called a stent. In some cases of unstable angina, heart surgery (coronary bypass surgery) may be needed. Generally, if you have mild stable angina that is controlled by medications, you may not need further treatments. If you're experiencing symptoms of chronic stable angina even after taking medications and making lifestyle changes, or if you're at higher risk of serious heart disease, your doctor may recommend angioplasty or coronary bypass surgery. Making a decision on how to treat your angina can be difficult, but knowing the benefits and risks of stents and medications may help you decide.
Cancer, also called malignancy, is an abnormal growth of cells. There are more than 100 types of cancer, including breast cancer, skin cancer, lung cancer, colon cancer, prostate cancer, and lymphoma. Symptoms vary depending on the type. Cancer treatment may include chemotherapy, radiation, and/or surgery.

Such foods include carrots, eggplant, cauliflower, green beans, broccoli, peppers, onions, lettuce, zucchini, tomatoes, peanuts and walnuts. These foods are generally safe for you to eat at each meal without spiking your blood sugar.

Intelligent People Have Fewer Friends, Here's Why...

The Babies Hooked On Heroin |
Nelson syndrome refers to a spectrum of symptoms and signs arising from an adrenocorticotropin (ACTH)–secreting pituitary macroadenoma after a therapeutic bilateral adrenalectomy. The spectrum of clinical features observed relates to the local effects of the tumor on surrounding structures, the secondary loss of other pituitary hormones, and the effects of the high serum concentrations of ACTH on the skin. [1] The first case was reported by Nelson et al in 1958. [2]
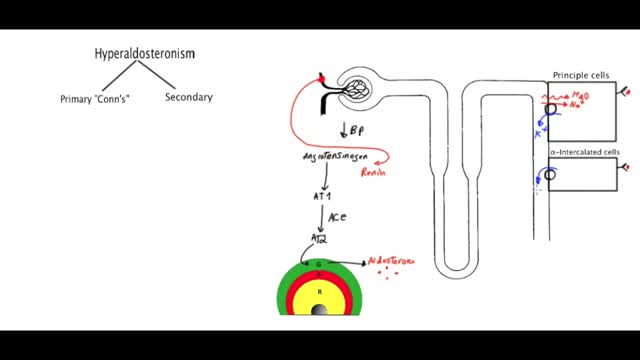
Primary aldosteronism, also known as primary hyperaldosteronism or Conn's syndrome, is excess production of the hormone aldosterone by the adrenal glands resulting in low renin levels. Often it produces few symptoms. Most people have high blood pressure which may cause poor vision or headaches.

What Happens When You're In a Coma?
The average human digestive tract is home to as many as 1,000 species of microorganisms. Most of them are harmless -- or even helpful -- under normal circumstances. But when something upsets the balance of these organisms in your gut, otherwise harmless bacteria can grow out of control and make you sick. One of the worst offenders is a bacterium called Clostridium difficile(C. difficile, or C. diff). As the bacteria overgrow they release toxins that attack the lining of the intestines, causing a condition called Clostridium difficilecolitis.

Blepharoplasty


