Top videoer

Dr. Linder is removing a patients breast implants after having five breast augmentations from three previous surgeons. She has baker 4 capsular contracture and is look forward to having them removed. The most common reasons for removing a breast implant include; heath reasons such as back pain, reoccurring complications and the desire for a different shape or size. For implant removal surgery, Dr. Linder makes an inframammary incision (along the breast crease). The implant can be removed intact, or it may need to be punctured before removal. An antibiotic solution is used to irrigate the breast pocket after implant removal. For more information about breast implant removal go to www.implantremoval.net or call Dr. Linder's office at 310-275-4513

Video of brain surgery

Toilet Training Boys, Training Potty, Best Way To Potty Train, What Age Do You Potty Train
http://potty-training-fast.good-info.co
Wanna have some fun imagining life without diapers?
Imagine if your child would disappear on their own
one minute and all of a sudden the next minute you
hear the toilet flush and the sink start to run.
Can you imagine it?
Life becomes so much easier the second your child
becomes potty trained and you start to wonder why
you didn't just get it over with sooner...
Would you start potty training right this weekend
if I handed you a guide that guaranteed to get your
child out of diapers in just 3 days?
Click the link below to check it out
http://potty-training-fast.good-info.co
Subscribe to our channel
http://potty-training-fast.blogspot.com/
https://www.youtube.com/watch?v=ck-4RTvP5F4
Toilet Training Boys, Training Potty, Best Way To Potty Train, What Age Do You Potty Train,
3day potty training,
toilet training tips for girls,
how to do potty training,
best potty training book,
potty training boys the easy way,
potty training activities,
how to potty training,
potty training video for toddlers,
when do you potty train,
how to potty train a kid,
potty training at 18 months,
havanese potty training,
how to potty train your baby,

Dont worry sister!
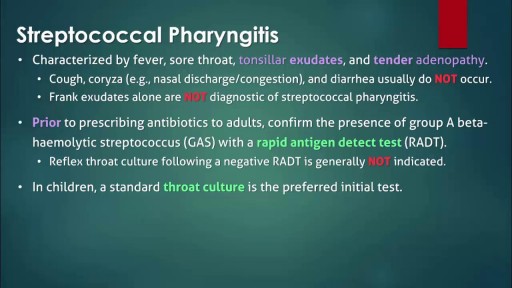
The infection is generally transmitted by direct contact with the mucus or sores of someone else with strep. Common symptoms include sore throat, fever, and swollen lymph nodes in the neck. Rarely, complications can involve the heart or kidneys. Treatment is important to reduce complications. Oral antibiotics like penicillin, amoxicillin, cephalexin, or azithromycin are commonly used. Other medicines such as acetaminophen or ibuprofen can help with pain and fever.

How to keep those creepy crawly lice from pestering your family’s scalps– tips on prevention and removal.

how to control arterial bleeding Learn more at http://www.ProTrainings.com

ATTENTION! 5 Warning Signs Of BREAST CANCER That Many Women Ignore!

Learn more about Merit Medical's ProGuide™ Chronic Dialysis
Adenomyosis is a condition in which the inner lining of the uterus (the endometrium) breaks through the muscle wall of the uterus (the myometrium). Adenomyosis can cause menstrual cramps, lower abdominal pressure, and bloating before menstrual periods and can result in heavy periods.

Amanda walks Chelsea through how to do the basics of a one leg squat, as she tries not to fall over. Do it at home, at work, or at the gym! No equipment needed! Check us out on Social Media! Facebook: https://www.facebook.com/striveptandperformance/ Instagram: https://www.instagram.com/striveptandperf/ Twitter: https://twitter.com/StrivePTandPerf Blog: http://www.strivept.ca/blog

Basic Surgical Instrumentation

Dr. Arthur Handal explains the differences patients can expect when their surgeon chooses to use either a needle or a cannula to inject facial fillers.

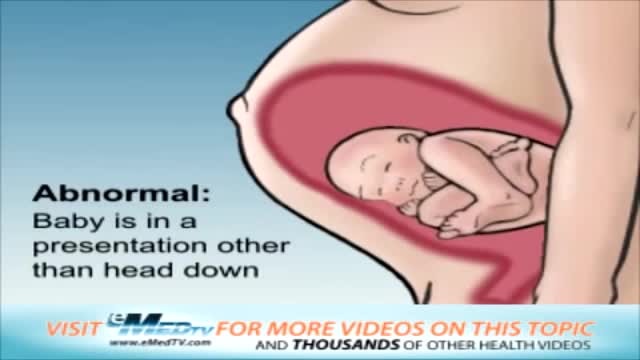
This video describes the various positions a baby may be in prior to delivery.

Menorrhagia is the medical term for menstrual periods with abnormally heavy or prolonged bleeding. Although heavy menstrual bleeding is a common concern, most women don't experience blood loss severe enough to be defined as menorrhagia. With menorrhagia, you can't maintain your usual activities when you have your period because you have so much blood loss and cramping. If you dread your period because you have such heavy menstrual bleeding, talk with your doctor. There are many effective treatments for menorrhagia. Symptoms Signs and symptoms of menorrhagia may include: Soaking through one or more sanitary pads or tampons every hour for several consecutive hours Needing to use double sanitary protection to control your menstrual flow Needing to wake up to change sanitary protection during the night Bleeding for longer than a week Passing blood clots larger than a quarter Restricting daily activities due to heavy menstrual flow Symptoms of anemia, such as tiredness, fatigue or shortness of breath

Blackheads, Cysts & Pimples

Hemorrhoids (HEM-uh-roids), also called piles, are swollen veins in your anus and lower rectum, similar to varicose veins. Hemorrhoids have a number of causes, although often the cause is unknown. They may result from straining during bowel movements or from the increased pressure on these veins during pregnancy.
Best Gynecomastia surgeon in India is Dr. Ajaya Kashyap, with over 20 years experience in breast surgeries. He is the only active Indian member in American Society of Plastic Surgeons. Contact us to find out about your gynecomastia treatment in Delhi, India, maintaining high international standards, having a U.S. board certified surgeon, and latest technology and surgical techniques, our offices offer very economical costing. Contact us today inquire about gynecomastia surgery cost, in Delhi. You are sent query using WhatsApp and website.
For further information, are available visit our website: http://www.bestgynecomastiaindia.com/
Your Query for Chat and call +91-9818369662, 9958221983 (WhatsApp)
