- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
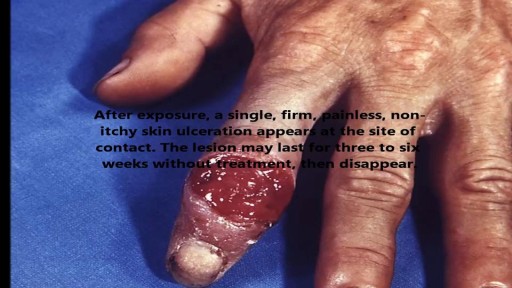
STDs are infections that are transmitted during vaginal, anal, and oral sex. They are very common and many people who have them don't show any symptoms.

http://www.landging.com/endocrine-system-animation.html
This endocrine system animation demonstrates mechanism of action of human body in 3D.

Median Sternotomy performed before open heart surgery !

http://www.landging.com/accident-animation-sports-injury-soccer.html
This accident animation demonstrates sports injury in soccer game.

The major elements of the cardiac exam include observation, palpation and, most importantly, auscultation (percussion is omitted). As with all other areas of the physical exam, establishing adequate exposure and a quiet environment are critical. Initially, the patient should rest supine with the upper body elevated 30 to 45 degrees. Most exam tables have an adjustable top. If not, use 2 or 3 pillows. Remember that although assessment of pulse and blood pressure are discussed in the vital signs section they are actually important elements of the cardiac exam.
Digoxin is derived from the leaves of a digitalis plant. Digoxin helps make the heart beat stronger and with a more regular rhythm. Digoxin is also used to treat atrial fibrillation, a heart rhythm disorder of the atria (the upper chambers of the heart that allow blood to flow into the heart).

1500 mg of sodium amounts to 0.75 teaspoons or 3.75 grams of salt per day, while 2300 mg amounts to one teaspoon or 6 grams of salt per day. Most people today are eating much more than that. The average intake of sodium is about 3400 mg, most of it coming from processed foods.
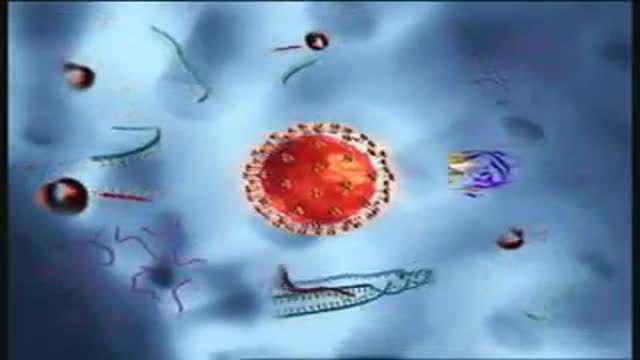
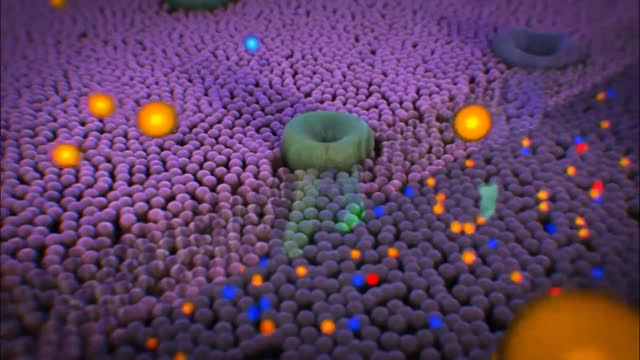
Binding and Fusion: HIV begins its life cycle
when it binds to a CD4 receptor and one of two
co-receptors on the surface of a CD4+
Tlymphocyte. The virus then fuses with the host
cell. After fusion, the virus releases RNA, its
genetic material, into the host cell.
Reverse Transcription: An HIV enzyme
called reverse transcriptase converts the singlestranded HIV RNA to double-stranded HIV DNA.
Integration: The newly formed HIV DNA
enters the host cell's nucleus, where an HIV
enzyme called integrase "hides" the HIV DNA
within the host cell's own DNA. The integrated
HIV DNA is called provirus. The provirus may
remain inactive for several years, producing few or
no new copies of HIV
Transcription: When the host cell receives a
signal to become active, the provirus uses a host
enzyme called RNA polymerase to create copies of
the HIV genomic material, as well as shorter
strands of RNA called messenger RNA (mRNA).
The mRNA is used as a blueprint to make long
chains of HIV proteins.
Assembly: An HIV enzyme called protease cuts
the long chains of HIV proteins into smaller
individual proteins. As the smaller HIV proteins
come together with copies of HIV's RNA genetic
material, a new virus particle is assembled.
Budding: The newly assembled virus pushes out
("buds") from the host cell. During budding, the new
virus steals part of the cell's outer envelope. This
envelope, which acts as a covering, is studded with
protein/sugar combinations called HIV
glycoproteins. These HIV glycoproteins are
necessary for the virus to bind CD4 and coreceptors. The new copies of HIV can now move
on to infect other cells.

Popping a Big Zit on the Face

A visual prosthesis, often referred to as a bionic eye, is an experimental visual device intended to restore functional vision in those suffering from partial or total blindness. In 1983 Joao Lobo Antunes, a Portuguese doctor, implanted a bionic eye in a person born blind.
http://www.drmarylupo.com/ Rosacea is sometimes called 'adult acne', but it's not. Over 14million Americans have Rosacea. For most, Rosacea is an embarrassing cyclical condition, coming and going.
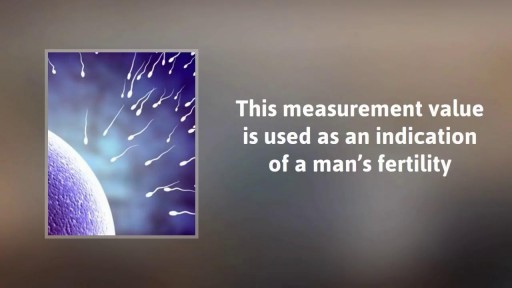
ormal sperm densities range from 15 million to greater than 200 million sperm per milliliter of semen. You are considered to have a low sperm count if you have fewer than 15 million sperm per milliliter or less than 39 million sperm total per ejaculate.

An appendectomy (sometimes called appendisectomy or appendicectomy (British English)) is the surgical removal of the vermiform appendix. This procedure is normally performed as an emergency procedure, when the patient is suffering from acute appendicitis. In the absence of surgical facilities, intravenous antibiotics are used to delay or prevent the onset of sepsis; it is now recognized that many cases will resolve when treated perioperatively. In some cases the appendicitis resolves completely; more often, an inflammatory mass forms around the appendix, causing transruptural flotation. This is a relative contraindication to surgery.
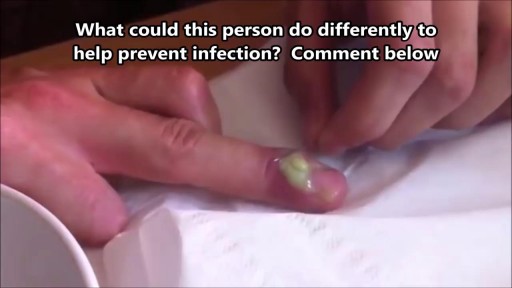
What Is a Paronychia (Nail Infection)? An infection that develops along the edge of the fingernail or toenail is called a paronychia (pear-ah-NIK-ee-ah). It is the most common hand infection and, if left untreated, can progress to a more severe infection of the entire finger or toe. Paronychia is distinguished from other infections such as onychomycosis and herpetic whitlow by its location and appearance.
Diabetic retinopathy is classified into two types: Non-proliferative diabetic retinopathy (NPDR) is the early stage of the disease in which symptoms will be mild or nonexistent. In NPDR, the blood vessels in the retina are weakened. ... Proliferative diabetic retinopathy (PDR) is the more advanced form of the disease.
Understanding Male Infertility

Oral sex is a commonly performed act of foreplay involving the kissing or licking of the genital area to pleasure a partner. However, it is sometimes stated that the act alone can increase the risk of throat cancer. Is this really the case?
Sex reassignment surgery for male-to-female involves reshaping the male genitals into a form with the appearance of, and, as far as possible, the function of female genitalia. Prior to any surgeries, patients usually undergo hormone replacement therapy (HRT), and, depending on the age at which HRT begins, facial hair removal. There are associated surgeries patients may elect to, including facial feminization surgery, breast augmentation, and various other procedures.

o you have an exercise routine that makes you feel absolutely awesome when you stick to it? Or a healthy eating pattern that makes you crackle with energy and vitality when you actually follow it. Well, today I’m sharing with you what makes me feel even more alive, energetic and vibrant than both of those… My daily sexual self-care practice.

Video of brain surgery
