- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Alzheimer Disease Effects

Blackheads, Cysts & Pimples

Baby Mucus Removal - Is This Right Way???

Scoliosis is a sideways curvature of the spine that occurs most often during the growth spurt just before puberty. While scoliosis can be caused by conditions such as cerebral palsy and muscular dystrophy, the cause of most scoliosis is unknown. Most cases of scoliosis are mild, but some children develop spine deformities that continue to get more severe as they grow. Severe scoliosis can be disabling. An especially severe spinal curve can reduce the amount of space within the chest, making it difficult for the lungs to function properly. Children who have mild scoliosis are monitored closely, usually with X-rays, to see if the curve is getting worse. In many cases, no treatment is necessary. Some children will need to wear a brace to stop the curve from worsening. Others may need surgery to keep the scoliosis from worsening and to straighten severe cases of scoliosis.
http://endyourdepression.plus101.com ---Depression Alternative Medicine Remedies. Learn more about your own, unique depression symptoms and pin-point exactly which type of depression you are suffering from. Accurately discover what is causing your depression... and why it keeps coming back no matter which drugs you take or which treatments you try. Uncover the simple methods that allow you to switch your mind away from depression and towards real happiness. Gain real insight into why most depression treatments only make your symptoms worse. Depression Alternative Medicine Remedies depressive major disorder symptoms signs medication treatment clinical causes anxiety teen help hurts self test medicine antidepression types anxiety severe
Alcoholic hepatitis can occur in people who drink heavily for many years. Symptoms include yellow skin and eyes along with increasing belly size due to fluid accumulation. Treatment involves hydration, nutritional care, and stopping alcohol use. Steroid drugs can help reduce liver inflammation.
Worlds Most Amazing Medical Case

Initial treatment of a deviated septum may be directed at managing the symptoms of the tissues lining the nose, which may then contribute to symptoms of nasal obstruction and drainage. Your doctor may prescribe: Decongestants. Decongestants are medications that reduce nasal tissue swelling, helping to keep the airways on both sides of your nose open. Decongestants are available as a pill or as a nasal spray. Use nasal sprays with caution, however. Frequent and continued use can create dependency and cause symptoms to be worse (rebound) after you stop using them. Decongestants have a stimulant effect and may cause you to be jittery as well as elevate your blood pressure and heart rate. Antihistamines. Antihistamines are medications that help prevent allergy symptoms, including obstruction and runny nose. They can also sometimes help nonallergic conditions such as those occurring with a cold. Some antihistamines cause drowsiness and can affect your ability to perform tasks that require physical coordination, such as driving. Nasal steroid sprays. Prescription nasal corticosteroid sprays can reduce inflammation in your nasal passage and help with obstruction or drainage. It usually takes from one to three weeks for steroid sprays to reach their maximal effect, so it is important to follow your doctor's directions in using them. Medications only treat the swollen mucus membranes and won't correct a deviated septum.

The is a time lapse video animation of a complicated ear infection with a ruptured eardrum causing drainage with eventual healing. The video also shows why a period of hearing loss and clogged/muffled ear sensation may occur.
Type 2 Diabetes Animation 3D
How to Know If You Have Diabetes

The condition is caused by a blockage in the lymphatic system, part of the immune and circulatory systems. Lymphedema is most commonly caused by lymph node removal or damage due to cancer treatment. The main symptom is swelling in an arm or leg that may be accompanied by pain or discomfort. Exercise, wrapping, massage, and compression can help.
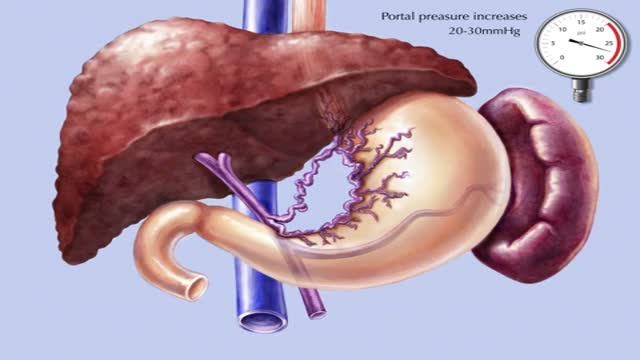
Transjugular intrahepatic portosystemic shunt or transjugular intrahepatic portosystemic stent shunting (commonly abbreviated as TIPS or TIPSS) is an artificial channel within the liver that establishes communication between the inflow portal vein and the outflow hepatic vein.

Diseases and Disorders of the Nails
Providing information on the Atherosclerosis and its complex biological process: it is the idea of this medical video dedicated to the prevention of the cardiovascular risks of diseases.

Are most spiders poisonous? The majority of the 3,000 spiders in the United States aren’t poisonous. Even if most spiders did bite, their fangs are too small or weak to puncture human skin. Their bites may leave itchy, red wounds that heal within a week or so. The spiders that do manage to bite through our skin and insert toxic venom can cause serious health complications. Read on to learn what spider bites look like, what spider varieties leave certain bites, and how to treat spider bites. What do spider bites look like? Identifying a spider bite is easier if you saw the spider that bit you, but it’s possible that you won’t notice the wound until hours later. Look for things like: swelling a red welt skin damage any troubling symptoms that accompany the bite Other possible symptoms that may accompany a spider bite include: itching or rash pain around the area of the bite muscle pain or cramping blister that’s red or purple in color sweating difficulty breathing headache nausea and vomiting fever chills anxiety or restlessness rashes swollen lymph glands high blood pressure Spider bites often take longer to heal than other insect bites, and they may affect skin tissues. It’s important to keep the bite clean to reduce the risk of infection. How to treat a spider bite at home In some cases, you can treat spider bites at home. For nonvenomous spider bites, follow these steps: Apply an ice pack on and off the bite for 10 minutes at a time. Elevate the area to reduce swelling. Take an antihistamine, such as diphenhydramine (Benadryl), to help with itching. Clean the area with soap and water to prevent infection. Apply antibiotic ointment to the area if blisters develop. Seek medical attention if you’re showing symptoms of a spider bite or if the symptoms don’t go away over time. Always seek medical attention if you suspect you’ve been bitten by one of the following species: brown recluse black widow hobo spider tarantula Brazilian wandering spider

The inflatable penile prosthesis consists of two attached cylinders -- a reservoir and a pump -- which are placed surgically in the body. The two cylinders are inserted in the penis and connected by tubing to a separate reservoir of saline. The reservoir is implanted under the rectus muscles in the lower abdomen. The Coloplast Titan Touch inflatable penile prosthesis is a self-contained, fluid-filled system made from Bioflex and silicone.
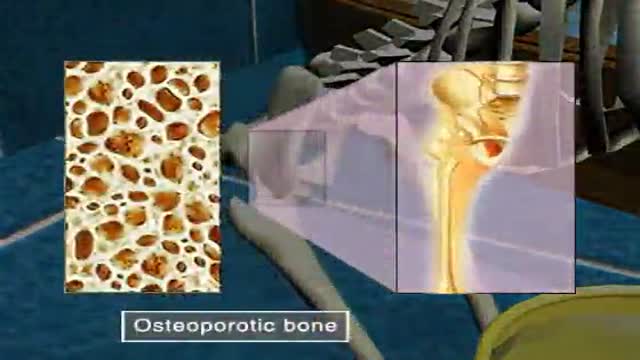
Osteoporosis
A penile prosthesis is another treatment option for men with erectile dysfunction (ED). These devices are either malleable or inflatable. The simplest type of prosthesis consists of a pair of malleable (bendable) rods surgically implanted within the erection chambers of the penis. With this type of implant the penis is always semi-rigid and merely needs to be lifted or adjusted into the erect position to initiate sex. Today, many men choose a hydraulic, inflatable prosthesis, which allows a man to have an erection whenever he chooses and is much easier to conceal. It is also more natural.
this animated surgery showing management of bone defects with the Precice Lengthening-Compression IM nail
