- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Combined Spinal-Epidural Obstetric Anesthesia

Follicle removal (Bascon's technique)

Female to Male gender confirming top surgery video : "Double Incision" Technique.

Watch that video of a Very Large Mole Removal Surgery

Watch that 200 lb Tumor in Man's Body Removal Surgery

Liver Metastasis Resection. A Technique That Makes It Easier. Authors: de Santibañes E, Sánchez Clariá R, Palavecino M, Beskow A, Pekolj J. Background: Liver resection is the only therapeutic option that achieves long-term survival for patients with hepatic metastases. We propose a tech...nique that causes traction and counter traction on the resection area, thus easily exposing the structures to be ligated. Since the parenchyma protrudes like a cork from a bottle we named this procedure “Corkscrew Technique”. Objective: To describe an original surgical technique to resect liver metastases. Technique: We delimite the resection area at 2 cm from the tumor. We place separated stitches, in a radiate way. The needle diameter must allow passing far from the deepest margin of the tumor. The stitches must be tractioned all together to separate the tumor from the normal parenchyma. Material and Methods: Between years 1983 and 2006, we perform 1270 liver resection. We used the corkscrew technique like only procedure in 612 patients whereas in 129 patients we associated it to an anatomic resection. Results: Mortality was 1%. Morbidity was 16% with a reoperation rate of 3%. Conclusions: The Corkscrew Technique is simple and safe, it spares surgical time, avoids blood loss, ensures free tumor margins and it is easy to perform.
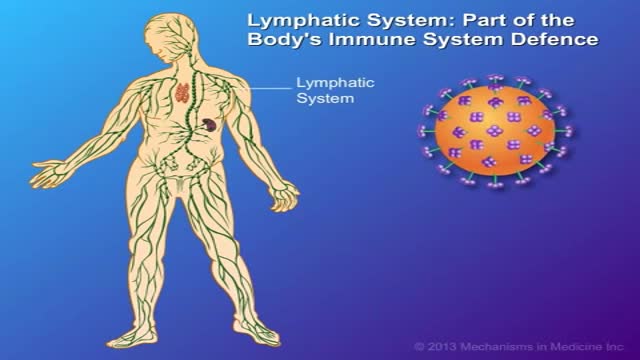
CD4 T-cells (a type of white blood cell) are important to your body's defence against infections. This animation describes how your immune system is weakened by the HIV virus, which targets CD4 T-cells and leads to their gradual decline in number. Low to very low levels of CD4 cells put you at risk for 'opportunistic infections' that take advantage of the body's weakened immune system.
Bone Repair Animation

Bruce had a stroke 2 years ago. Then, he broke his hip. The stroke affected his right side, and he has had limited mobility and was using a walker for recovery, Bruce could only walk with breaks and was hunched over. The GlideTrak opened Bruce's posture and allowed him to breath better and allowed for over 25 minutes of walking exercise, greatly increasing the Patients self-confidence and at the end he was actually able to stand on his own feet, with the straps as guides, whereas this was not possible before his sessions on the GlideTrak. clean, water-damp cloth. Repeat application procedure as needed.

Ligation around a hemostatic Clamp
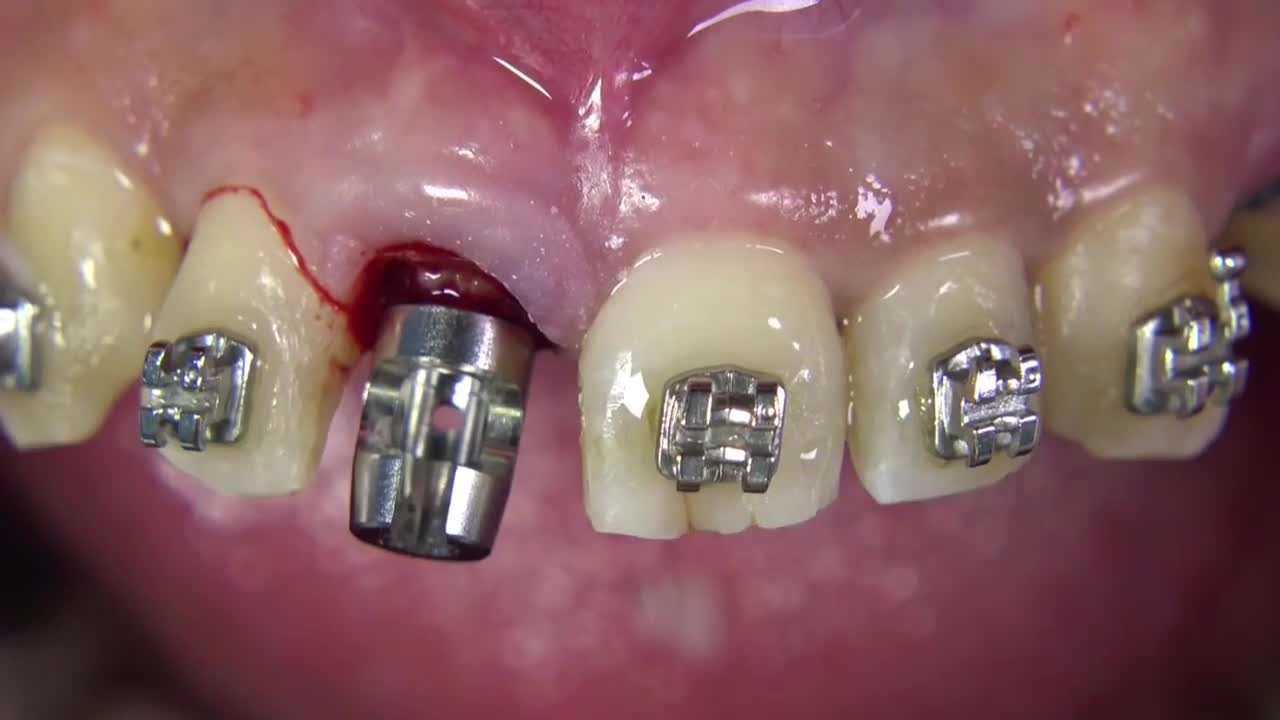
Benex II Surgical Extraction System

Thanks to a new, state-of-the-art procedure for total knee replacement developed by surgeons at the Detroit Medical Center's Sinai-Grace Hospital, the rehabilitation time for patients has been reduced from six months to six weeks. ~ Detroit Medical Center
Aortic Valve-Sparing Operation in a Patient with Aortic Root Aneurysm using a new Prosthesis for Anatomical Reconstruction of the Sinuses of Valsalva

This video shows the many alternatives of hysterectomy and the advantages of each method

Comprehensive physical examination

A tapeworm is a ribbon-shaped parasite that lives in human or animal intestines. They are uncommon in developed countries. There are a number of different types which all have slightly different life cycles. Tapeworm infection can come from animals such as pigs, sheep, cattle, fish, dogs and cats. Eating undercooked food contaminated with tapeworm cysts and eggs causes the infection. Tapeworm eggs are shed in stools and it is possible for infection to spread from person to person through the oral/anal route.
An excerpt from the award-winning documentary “Exposure: Environmental Links to Breast Cancer” about the effects of radiation. Featuring Olivia Newton-John, Dr. Rosalie Bertell and Dr. Susan Love.
A clue cell appears smudged, with indistinct contents and fuzzy, poorly defined borders.

Triangular flap fornix based trabeculectomy in POAG using MMC

This video demonstrates pelvic adhesions found in a patient with endometriosis during laparoscopic surgery.
