סרטונים מובילים

This video clips shows a tubal ligation (sterilization) performed on a female using a fallopian ring applicator

What are blackheads? Blackheads are small bumps that appear on your skin due to clogged hair follicles. These bumps are called blackheads because the surface looks dark or black. Blackheads are a mild type of acne that usually form on the face, but they can also appear on the following body parts: back chest neck arms shoulders Acne affects nearly 50 million Americans and is the most common skin disorder in the United States, according to the American Academy of Dermatology. What do blackheads look like? What causes blackheads? Blackheads form when a clog or plug develops in the opening of hair follicles in your skin. Each follicle contains one hair and a sebaceous gland that produces oil. This oil, called sebum, helps keep your skin soft. Dead skin cells and oils collect in the opening to the skin follicle, producing a bump called a comedo. If the skin over the bump stays closed, the bump is called a whitehead. When the skin over the bump opens, exposure to the air causes it to look black and a blackhead forms. Some factors can increase your chances of developing acne and blackheads, including: producing too much body oil the buildup of the Propionibacterium acnes bacteria on the skin irritation of the hair follicles when dead skins cells don’t shed on a regular basis undergoing hormonal changes that cause an increase in oil production during the teen years, during menstruation, or while taking birth control pills taking certain drugs, such as corticosteroids, lithium, or androgens Some people believe that what you eat or drink can affect acne. Dairy products and foods that increase blood sugar levels, such as carbohydrates, may play a part in triggering acne, but researchers aren’t convinced that there’s a strong connection. ADVERTISING What are symptoms of blackheads? Because of their dark color, blackheads are easy to spot on the skin. They’re slightly raised, although they aren’t painful because they aren’t inflamed like pimples. Pimples form when bacteria invade the blockage in the hair follicle, causing redness and inflammation. How are blackheads treated? Over-the-counter (OTC) treatments Many acne medications are available at drug and grocery stores and online without a prescription. These medications are available in cream, gel, and pad form and are put directly on your skin. The drugs contain ingredients such as salicylic acid, benzoyl peroxide, and resorcinol. They work by killing bacteria, drying excess oil, and forcing the skin to shed dead skin cells. Prescription medications If OTC treatment doesn’t improve your acne, your doctor may suggest that you use stronger prescription medications. Medications that contain vitamin A keep plugs from forming in the hair follicles and promote more rapid turnover of skin cells. These medications are applied directly to your skin and can include tretinoin, tazarotene, or adapalene. Your doctor may also prescribe another type of topical medication that contains benzoyl peroxide and antibiotics. If you have pimples or acne cysts in addition to your blackheads, this type of medication may be particularly helpful. Manual removal Dermatologists or specially trained skin care professionals use a special instrument called a round loop extractor to remove the plug causing the blackhead. After a small opening is made in the plug, the doctor applies pressure with the extractor to remove the clog. Microdermabrasion During microdermabrasion, a doctor or skin care professional uses a special instrument that contains a rough surface to sand the top layers of your skin. Sanding the skin removes clogs that cause blackheads. Chemical peels Chemical peels also remove clogs and get rid of the dead skins cells that contribute to blackheads. During a peel, a strong chemical solution is applied to the skin. Over time, the top layers of the skin peel off, revealing smoother skin underneath. Mild peels are available over the counter, while stronger peels are performed by dermatologists or other skincare professionals. Laser and light therapy Laser and light therapies use tiny beams of intense light to decrease oil production or kill bacteria. Both lasers and light beams reach below the surface of the skin to treat blackheads and acne without damaging the top layers of the skin. How can blackheads be prevented? You can prevent blackheads without spending a lot of money by trying a few of the following ideas: Wash regularly Wash your face when you wake up and before you go to bed to remove oil buildup. Washing more than twice each day can irritate your skin and make your acne worse. Use a gentle cleanser that doesn’t make your skin red or irritated. Some acne cleansing products have antibacterial ingredients that kill P. acnes bacteria. Consider washing your hair every day, too, particularly if it’s oily. Hair oils can contribute to clogged pores. It’s also important to wash your face after you eat oily foods such as pizza, because oil from these foods can clog pores. Use oil-free products Any product that contains oil can contribute to new blackheads. Choose oil-free or noncomedogenic makeup, lotions, and sunscreens to avoid making your problem worse. Try an exfoliating product Exfoliating scrubs and masks remove dead skin cells from your face and can help reduce blackheads. Look for products that don’t irritate your skin.

A video showing impaled objects

The external jugular vein receives the greater part of the blood from the exterior of the cranium and the deep parts of the face, being formed by the junction of the posterior division of the retromandibular vein with the posterior auricular vein.


A man set to become the world’s first head transplant patient has scheduled the procedure for December 2017. Valery Spiridonov, 30, was diagnosed with a genetic muscle-wasting condition called Werdnig-Hoffmann disease, and volunteered for the procedure despite the risks involved, Central European News (CEN) reported. “When I realized that I could participate in something really big and important, I had no doubt left in my mind and started to work in this direction,” Spiridonov, a Russian computer scientist, told CEN. “The only thing I feel is the sense of pleasant impatience, like I have been preparing for something important all my life and it is starting to happen.”

There are a number of different causes of vertigo. Vertigo can be defined based upon whether the cause is peripheral or central. Central causes of vertigo arise in the brain or spinal cord while peripheral vertigo is due to a problem within the inner ear. The inner ear can become inflamed because of illness, or small crystals or stones found normally within the inner ear can become displaced and cause irritation to the small hair cells within the semicircular canals, leading to vertigo. This is known as benign paroxysmal positional vertigo (BPPV).
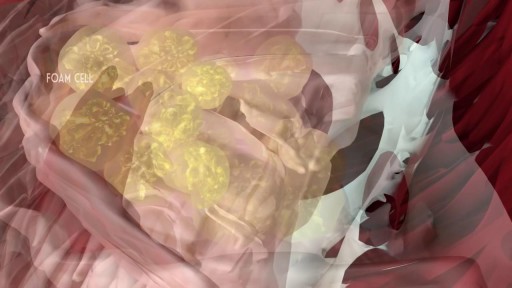
Atherosclerosis is a process in which blood, fats such as cholesterol, and other substances build up on your artery walls. Eventually, deposits called plaques may form. The deposits may narrow — or block — your arteries. These plaques can also rupture, causing a blood clot.

This Unorthodox Procedure Makes Short People A Foot Taller

Knee replacement involves replacing a knee joint that has been damaged or worn away, usually by arthritis or injury. Find out more here: http://bit.ly/MAdfmE
The content is intended for general information only and does not replace the need for personal advice from a qualified health professional.

Dr. David Rivadeneira from Stony Brook University in Stony Brook, NY will host a panel discussion on how to obtain improved outcomes during open surgery through the application of advanced techniques and technologies, including the new LigaSure Impact™ instrument. "It provides excellent and reliable hemostasis on major blood vessels, but the big advancement is that it is faster than traditional techniques and leaves no foreign material behind."
The program will begin with a brief introduction of the topic, followed by video presentation of two procedures, a right hemicolectomy and a sigmoid colectomy. Dr. Rivadeneira will discuss the techniques that he uses. "You'll be able to see the impact of applying multifunctional energy-based instruments to enable rapid and reliable dissection of the mesentery and ligation of colonic blood supply. This is particularly evident on tough diverticular cases, where it works very well with complicated tissue." Joining Dr. Rivadeneira, to review and discuss the cases, will be Dr. Sang Lee from Weill Cornell Medical College, NY.

Another video of Dr.Vijay C. Bose from Apollo Speciality Hospital chennai perform Birmingham Hip Resurfacing Surgery procedure for a case of Avascular necrosis.The NCP ( Neck Capsule Preserving) approach is being used. Total hip replacement, hip resurfacing simply shaves and caps a few centimeters of bone within the joint. The bone-conserving approach of the Birmingham Hip Resurfacing System.
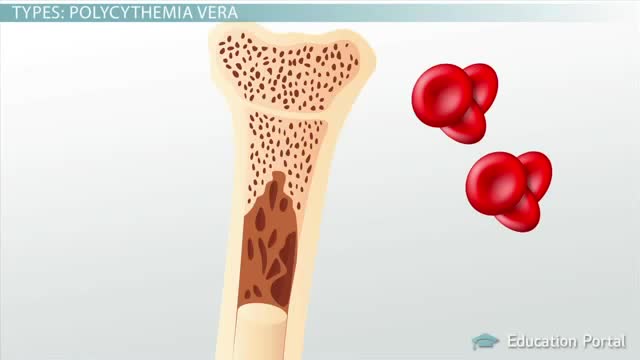
Polycythemia vera (pol-e-sigh-THEE-me-uh VEER-uh) is a slow-growing type of blood cancer in which your bone marrow makes too many red blood cells. Polycythemia vera may also result in production of too many of the other types of blood cells — white blood cells and platelets. These excess cells thicken your blood and cause complications, such as such as a risk of blood clots or bleeding. Polycythemia vera isn't common. It usually develops slowly, and you may have it for years without noticing signs or symptoms. Often, polycythemia vera is found during a blood test done for some other reason. Without treatment, polycythemia vera can be life-threatening. However, with proper medical care, many people experience few problems related to this disease. Over time, there's a risk of progressing to more-serious blood cancers, such as myelofibrosis or acute leukemia.

Anemia is a medical condition in which the red blood cell count or hemoglobin is less than normal. The normal level of hemoglobin is generally different in males and females. For men, a normal hemoglobin level is typically defined as a level of more than 13.5 gram/100 ml, and in women as hemoglobin of more than 12.0 gram/100 ml. These definitions may vary slightly depending on the source and the laboratory reference used. Continue Reading

Dr. Leo Maguire, a Mayo Clinic ophthalmologist, explains how laser-assisted in situ keratomileusis (LASIK) eye surgery can correct common vision problems.
This interview originally aired Jan. 26, 2019.
To learn more about LASIK surgery, visit: https://www.mayoclinic.org/tests-procedures/lasik-eye-surgery/about/pac-20384774?mc_id=us&utm_source=newsnetwork&utm_medium=l&utm_content=content&utm_campaign=mayoclinic&geo=national&placementsite=enterprise&cauid=100721&_ga=2.112234244.1227307149.1547427243-1780934405.1469629163

See what it’s like to get LASIK eye surgery from Lisa Homsy’s perspective. Keep watching until the end to see the final results!
USMLE Step 2 CS - Pediatric Diarrhea This is just preview video. To get full access please visit our website : www.usmletutoring.com

Start out with a visit to a doctor called a urologist. He'll give you a physical exam and ask you questions about your lifestyle and medical history, such as: Surgeries you've had Medications you take Your exercise habits Whether you smoke or take recreational drugs He may also have a frank discussion with you about your sex life, including any problems you've had or whether you have or ever had any STDs (sexually transmitted diseases). You'll probably be asked to give a sample of semen for analysis.
Among common cancers, pancreatic cancer has one of the poorest prognoses. Because pancreatic cancer often grows and spreads long before it causes any symptoms, only about 6% of patients are still alive five years after diagnosis. For some pancreatic patients, however, a complex surgery known as the Whipple procedure may extend life and could be a potential cure. Those who undergo a successful Whipple procedure may have a five-year survival rate of up to 25%.

OPAXIO Mechanism of Action
