Top Videos

Meckels Diverticulum

The abortion pill is a medicine called mifepristone that ends an early pregnancy.In general, it's used up to 70 days — 10 weeks — after the first day of a woman's last period. Patients over this mark can have an in-clinic abortion procedure.
A modified radical mastectomy is a procedure in which the entire breast is removed, including the skin, areola, nipple, and most axillary lymph nodes; the pectoralis major muscle is spared. Historically, a modified radical mastectomy was the primary method of treatment of breast cancer. [1, 2] As the treatment of breast cancer evolved, breast conservation has become more widely used. [3, 4] However, mastectomy still remains a viable option for women with breast cancer. [5, 6]

For both DCIS and invasive cancer, radiation therapy to the remaining breast tissue is generally recommended after surgery. A lumpectomy may also be called breast-conserving surgery, a partial mastectomy, quadrantectomy, or a segmental mastectomy. A mastectomy is the surgical removal of the entire breast.

Vaser high definition liposuction is used for reducing fat in obese patients but it can be also used for lipo contouring in parts such as legs, thighs, arms and legs. The much sought-after 6 pack abs is also possible through this wonderful technique. Whether it is a small problem area or a full body transformation that you are seeking, vaser high definition liposuction works in your favor and gives you amazing results that you will be proud to flaunt.

Mini Face Lift Surgery -- Short Scars -- No Anesthesia

This video is demonstrating how to correct the most common sacroiliac dysfunction and that is an anterior innominate rotation using a muscle energy technique

irregular, curved toenails. footwear that places a lot of pressure on the big toes, such as socks and stockings that are too tight or shoes that are too tight, narrow, or flat for your feet. toenail injury, including stubbing your toe, dropping something heavy on your foot, or kicking a ball repeatedly. poor posture. How can ingrowing toenails be prevented? Cut your nails straight across; do not cut them too short or too low at the sides. ... Keep your feet clean and dry. ... Avoid tight shoes and use cotton socks rather than synthetic. If you have diabetes, you should take extra care when cutting your nails:

Liver Transplant Surgery Explained

Chainsaw Accident! Lacerations, Cysts, Blackheads & Surgerys
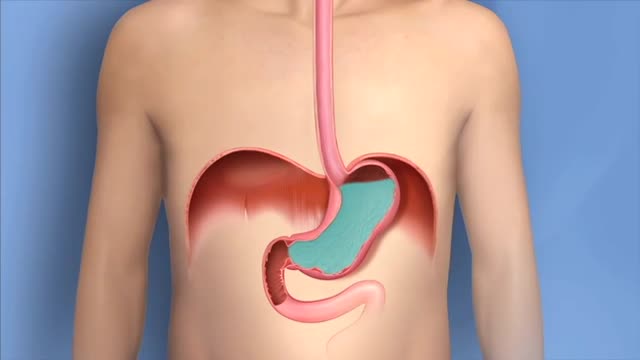
Heartburn is a burning pain in your chest, just behind your breastbone. The pain is often worse when lying down or bending over. Occasional heartburn is common and no cause for alarm. Most people can manage the discomfort of heartburn on their own with lifestyle changes and over-the-counter medications. Heartburn that is more frequent or interferes with your daily routine may be a symptom of a more serious condition that requires medical care
This animation describes the goals of inflammatory bowel disease (IBD) management and how patients can take an active role in managing their disease.
Non-Hodgkin's lymphoma, also called non-Hodgkin lymphoma, is cancer that originates in your lymphatic system, the disease-fighting network spread throughout your body. In non-Hodgkin's lymphoma, tumors develop from lymphocytes — a type of white blood cell. Non-Hodgkin's lymphoma is more common than the other general type of lymphoma — Hodgkin lymphoma. Many different subtypes of non-Hodgkin's lymphoma exist. The most common non-Hodgkin's lymphoma subtypes include diffuse large B-cell lymphoma and follicular lymphoma.
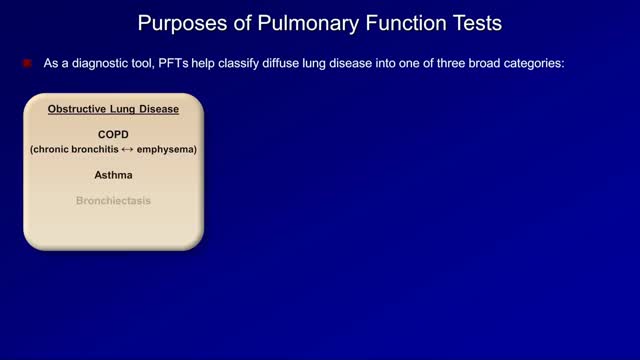
Pulmonary function tests are a broad range of tests that measure how well the lungs take in and exhale air and how efficiently they transfer oxygen into the blood. Spirometry measures how well the lungs exhale.

Womb Fight amazing
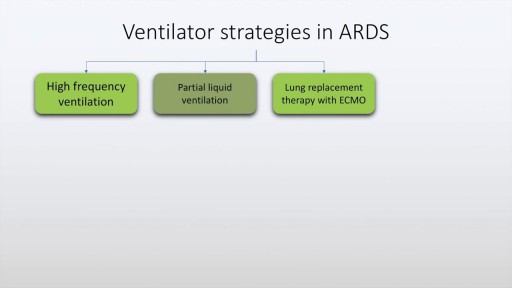
Acute respiratory distress syndrome is characterised by rapid onset dyspnea, bilateral infiltrates on chest x-ray and respiratory failure. This may be due to conditions which directly affect the lung such as pneumonia, aspiration and near drowning. It may also be due to indirect lung injury, as in conditions like sepsis, pancreatitis, trauma and poisoning. The diagnostic criteria of ARDS, often described as the Berlin criteria is discussed in this presentation along with various management aspects of ARDS including ventilation strategies and use of antibiotics and diuretics. Finally prognostic features and alternative strategies are also discussed.
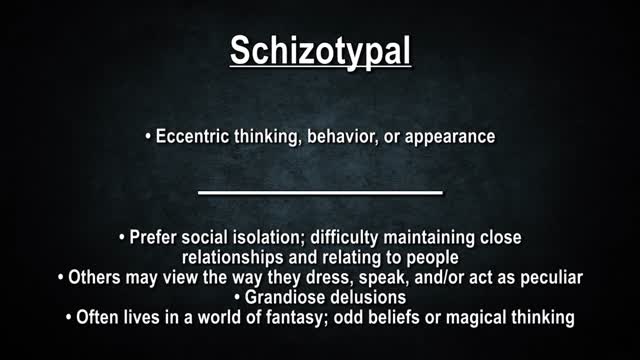
Personality disorders are a group of mental illnesses. They involve long-term patterns of thoughts and behaviors that are unhealthy and inflexible. The behaviors cause serious problems with relationships and work. People with personality disorders have trouble dealing with everyday stresses and problems. They often have stormy relationships with other people. The cause of personality disorders is unknown. However, genes and childhood experiences may play a role. The symptoms of each personality disorder are different. They can mild or severe. People with personality disorders may have trouble realizing that they have a problem. To them, their thoughts are normal, and they often blame others for their problems. They may try to get help because of their problems with relationships and work. Treatment usually includes talk therapy and sometimes medicine.
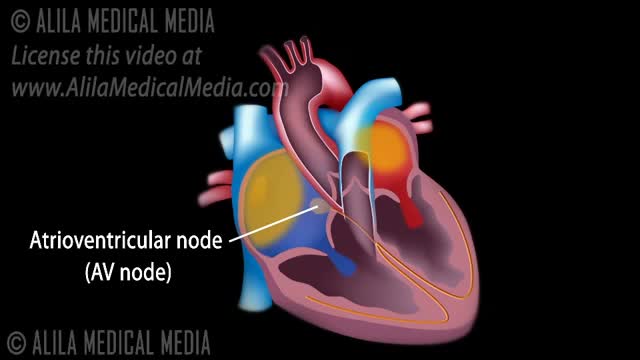
The normal electrical conduction in the heart allows the impulse that is generated by the sinoatrial node (SA node) of the heart to be propagated to (and stimulate) the cardiac muscle (myocardium). The myocardium contracts after stimulation.

Central vestibular nystagmus results from stimulation, injury, disease of the central vestibular pathways of the brainstem or the cerebellum, or lesion of the vestibular nuclei. It is typically a jerk nystagmus, which can be purely horizontal, vertical or torsional.
