- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Watch that video of Amputated Hand Reattachment Surgery
Acid Reflux Home Remedies, Acid Reflux Shortness Of Breath, Heartburn Nausea Fatigue, Acid Reflux. http://heartburn-acid-reflux.info-pro.co --- If you think the worst part about having Acid Reflux is heartburn and mild discomfort… You need to watch this video below IMMEDIATELY. In it, you’ll be shown the much darker side to your acid reflux… Something that over-the-counter and prescription drug manufacturers alike are spending billions to keep hidden from you… But that could soon cost you your LIFE...like it almost did to me. There are even over a dozen forms of cancer that can be traced back to your Acid Reflux, but the situation is not hopeless. Use this link now to see exactly what your biggest risk is…and how a highly unconventional method can rapidly and naturally CURE your Acid Reflux forever. Click Here: http://heartburn-acid-reflux.info-pro.co

The video will describe anatomial structures in a thoracic cavity as seen on a CT scan. Please see my website for disclaimer.
http://sweating-cure.info-pro.co/ --- Why Do I Sweat So Much, How To Stop Sweaty Armpits, How To Stop Your Hands From Sweating. The 4 Step Formula to Stop Sweating How to Stop Excessive Sweating in Minutes There is a simple 4 step formula you need to implement immediately if you want to finally end your excessive sweating and put a stop to the constant embarrassment. These 4 steps are absolutely essential if you’re having trouble controlling the endless perspiration. Don’t prolong the problem any longer. Take action with these simple steps right now. http://sweating-cure.info-pro.co/

Watch that video of Nasty Female Genital Infection

Watch that video to know What is Vaginal Discharge and how to Get Rid of it ?

This video is intended primarily for mothers in the developing world, but may be helpful to breastfeeding mothers worldwide.
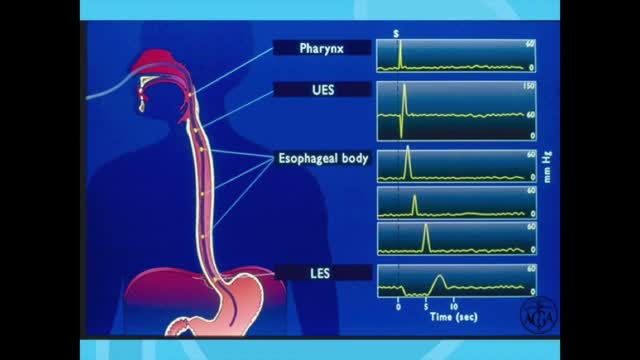
Esophageal manometry is a test used to measure the function of the lower esophageal sphincter (the valve that prevents reflux of gastric acid into the esophagus) and the muscles of the esophagus (see diagram). This test will tell your doctor if your esophagus is able to move food to your stomach normally.

Focal seizures (also called partial seizures [citation needed] and localized seizures) are seizures which affect initially only one hemisphere of the brain. [citation needed] The brain is divided into two hemispheres, each consisting of four lobes – the frontal, temporal, parietal and occipital lobes.

There are several things to consider when trying to decide between gastric bypass surgery and gastric sleeve surgery. Unlike the laparoscopic adjustable gastric band (Lap Band), these two operations are both permanent, reduce hunger, and lead to the highest percentage of weight loss. To properly compare gastric sleeve surgery to gastric bypass surgery we will examine the following data : Expected weight loss. Speed of weight loss. Time of surgery. Gastric bypass benefits over sleeve. Gastric sleeve benefits over bypass. Risk of complications. Surgeon skill and preference.
Renal artery stenosis is a narrowing of arteries that carry blood to one or both of the kidneys. Most often seen in older people with atherosclerosis (hardening of the arteries), renal artery stenosis can worsen over time and often leads to hypertension (high blood pressure) and kidney damage.
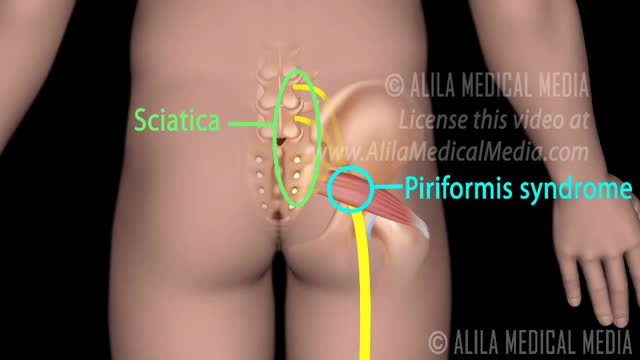
Piriformis syndrome refers to when the piriformis muscle irritates the sciatic nerve and caues pain along the back of the leg and foot.

Undiagnosed severe condition. 26th week of pregnancy. Sorry, I am reviewing the images, it is not a holoprosencephaly; more likely: corpus callosum agenesis. Please feedback

腹腔镜联合胆囊+阑尾切除术——普外寰潮网,汕头市第二人民医院

For both DCIS and invasive cancer, radiation therapy to the remaining breast tissue is generally recommended after surgery. A lumpectomy may also be called breast-conserving surgery, a partial mastectomy, quadrantectomy, or a segmental mastectomy. A mastectomy is the surgical removal of the entire breast.

A video showing the examination of femoral hernia.
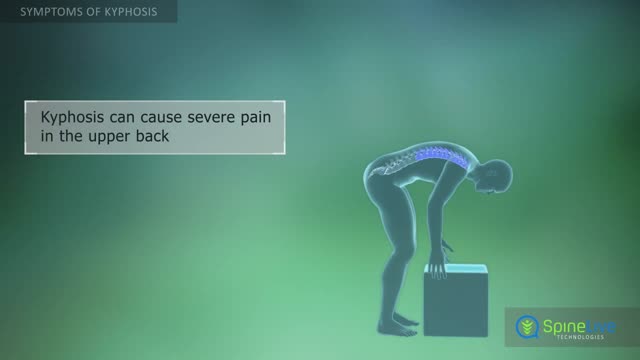
Kyphosis, also known as a round back or hunchback, is a condition in which the spine in the upper back has an excessive curvature. The upper back, or thoracic region of the spine, is supposed to have a slight natural curve.

The human brain is the command center for the human nervous system. It receives input from the sensory organs and sends output to the muscles. The human brain has the same basic structure as other mammal brains, but is larger in relation to body size than any other brains.

The products of a surgical abortion.

Graphic images focusing on the reconstruction of an ear after the removal of a long-standing skin cancer that this patient allowed to slowly grow over many years because he was afraid of what the surgery to remove might entail. Go to www.skincancercentre.com to learn more about the importance of the early diagnosis of skin cancer. BTW, when you put on your sunscreen, don't forget your ears, and wear a broad brimmed hat to cover this very vulnerable area of your anatomy. www.skincancercentre.com
