- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Mysterious massage from East Asia(CHINA).it can cure cure Erectile dysfunction,can let their life better.This video from mainland of China,so the language is Chinese mandarin.but you can see English show on the video too.Tiedang gong means kongfu of Iron penis&balls.

TV interview with Dr. Mostafa Yakoot, MD discussing his recently published study for efficacy of lettuce seed oil in patients with insomnia

Henry Anhalt DO FAAP
Ped Eddo

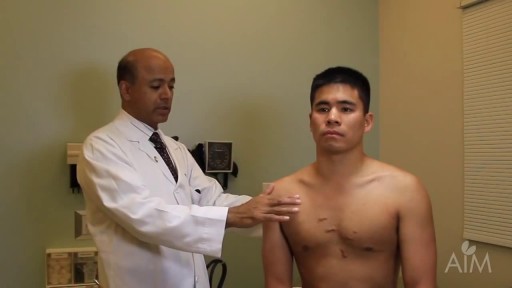
This video shows you how to examine the hand and wrist and how to identify common causes of pain.
This video clip is part of the FIFA Diploma in Football Medicine and the FIFA Medical Network. To enrol or to find our more click on the following link http://www.fifamedicalnetwork.com
The Diploma is a free online course designed to help clinicians learn how to diagnose and manage common football-related injuries and illnesses. There are a total of 42 modules created by football medicine experts. Visit a single page, complete individual modules or finish the entire course.
The network provides the opportunity for clinicians around the world to meet and share ideas relating to football medicine. Ask about an interesting case, debate current practice and discuss treatment strategies. Create a profile and log on to interact with other health professionals from around the globe.
This is not medical advice. The content is intended as educational content for health care professionals and students. If you are a patient, seek care of a health care professional.

Examination of the knee joint from the USMLE collection

We will show you what a sports hernia examination (aka athletic pubalgia, gilmore's groin, lower abdominal pain) and rule out a diagnosis of hip impingement. Rehab exercises are suggested based on the results.
If you're experiencing any of these symptoms, don't hesitate to schedule a sports hernia examination. I can help you determine the best treatment plan to promote your recovery and avoid future injury. Subscribe to my channel to stay updated on the latest medical news and tips!
If you would like to know more about sports hernias and other diagnoses for front of hip, groin, adductor and lower abdominal strain, watch our detailed webinar here: https://bit.ly/37thtNF
For treatment, come visit us or schedule a virtual session. www.p2sportscare.com
Costa Mesa CA 715-502-4243
#sportshernia #abdominal #hippain
Sports Hernia Diagnosis
What Is A Sports Hernia?
A sports hernia is tearing of the transversalis fascia of the lower abdominal or groin region. A common misconception is that a sports hernia is the same as a traditional hernia. The mechanism of injury is rapid twisting and change of direction within sports, such as football, basketball, soccer and hockey.
The term “sports hernia” is becoming mainstream with more professional athletes being diagnosed. The following are just to name a few:
Torii Hunter
Tom Brady
Ryan Getzlaf
Julio Jones
Jeremy Shockey
If you follow any of these professional athletes, they all seem to have the same thing in common: Lingering groin pain. If you play fantasy sports, this is a major headache since it seems so minor, but it can land a player on Injury Reserve on a moments notice. In real life, it is a very frustrating condition to say the least. It is hard to pin point, goes away with rest and comes back after activity, but is hardly painful enough to make you want to stop. It lingers and is always on your mind. And if you’re looking for my step-by-step sports hernia rehab video course here it is.
One the best definitions of Sport hernias is the following by Harmon:
The phenomena of chronic activity–related groin pain that it is unresponsive to conservative therapy and significantly improves with surgical repair.”
This is truly how sports hernias behave in a clinical setting. It is not uncommon for a sports hernia to be unrecognized for months and even years. Unlike your typical sports injury, most sports medicine offices have only seen a handful of cases. It’s just not on most doctors’ radar. The purpose of this article is not only to bring awareness about sports hernias, but also to educate.
Will you find quick fixes in this article for sports hernia rehab?
Nope. There is no quick fix for this condition, and if someone is trying to sell you one, they are blowing smoke up your you-know-what.
Is there a way to decrease the pain related to sports hernias?
Yes. Proper rehab and avoidance of activity for a certain period of time will assist greatly, but this will not always stop it from coming back. Pain is the first thing to go and last thing to come. Do not be fooled when you become pain-free by resting it. Pain is only one measure of improvement in your rehab. Strength, change of direction, balance and power (just to name a few) are important, since you obviously desire to play your sport again. If you wanted to be a couch potato, you would be feeling better in no time. Watching Sports Center doesn’t require any movement.
Why is this article so long?
There is a lot of information on sports hernias available to you on the web. However, much of the information is spread out all over the internet and hard for athletes to digest due to complicated terminology. This article lays out the foundational terminology you will need to understand what options you have with your injury. We will go over anatomy, biomechanics, rehab, surgery, and even the fun facts. The information I am using is from the last ten years of medical research, up until 2016. We will be making updates overtime when something new is found as well. So link to this page and share with friends. This is the best source for information on sports hernias you will find.
Common Names (or Aliases?) for Sports Hernias
Sportsman’s Hernia
Athletic Pubalgia
Gilmore’s Groin
How Do You Know If You Have A Sports Hernia?
Typical athlete characteristics:
Male, age mid-20s
Common sports: soccer, hockey, tennis, football, field hockey
Motions involved: cutting, pivoting, kicking and sharp turns
Gradual onset
How A Sports Hernia Develops
Chronic groin pain typically happens over time, which is why with sports hernias, we do not hear many stories of feeling a “pop” or a specific moment of injury. It is the result of “overuse” mechanics stemming from a combination of inadequate strength and endurance, lack of dynamic control, movement pattern abnormalities, and discoordination of motion in the groin area.
#SPORTSHERNIAEXAM #california
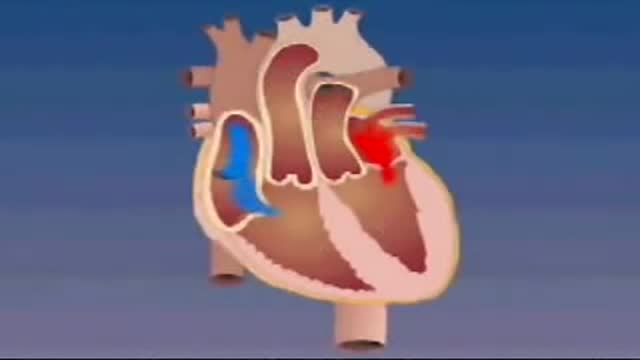
Transposition of the great arteries is a serious but rare heart defect present at birth (congenital), in which the two main arteries leaving the heart are reversed (transposed). Transposition of the great arteries changes the way blood circulates through the body, leaving a shortage of oxygen in blood flowing from the heart to the rest of the body. Without an adequate supply of oxygen-rich blood, the body can't function properly and your child faces serious complications or death without treatment.
http://www.wss4m.com/vb

Biliary Colic Examination

Intramedullary nailing of the tibia with suprapatellar entry and semi-extended positioning makes it technically easier to nail the proximal and distal fractures. The purpose of this article was to describe a simple method for suprapatellar nailing (SPN). A step-by-step run through of the surgical technique is described, including positioning of the patient. There are as yet only a few clinical studies that illustrate the complications with this method, and there has been no increased frequency of intraarticular damage. Within the body of the manuscript, information is included about intraarticular damage and comments with references about anterior knee pain.

Penile implants are devices placed inside the penis to allow men with erectile dysfunction (ED) to get an erection. Penile implants are typically recommended after other treatments for ED fail. There are two main types of penile implants, semirigid and inflatable.

Mitral valve surgery is surgery to either repair or replace the mitral valve in your heart. Blood flows from the lungs and enters a pumping chamber of the heart called the left atrium. The blood then flows into the final pumping chamber of the heart called the left ventricle. The mitral valve is located between these two chambers. It makes sure that the blood keeps moving forward through the heart. You may need surgery on your mitral valve if: The mitral valve is hardened (calcified). This prevents blood from moving forward through the valve. The mitral valve is too loose. Blood tends to flows backward when this occurs. Minimally invasive mitral valve surgery is done through several small cuts. Another type of operation, open mitral valve surgery requires a larger cut.

Carotid Stenosis and what it means. The detection and treatment of carotid artery disease for the prevention of stroke is one of the most effective treatments in all of medicine.
USMLE Step 2 CS - Numbness Weakness Full Video

mammoplasty, is a surgical enhancement procedure to accentuate the size and shape of a woman’s breasts. While breast augmentation will make the breasts larger, the surgery will not move the breasts closer together or lift sagging breasts. Breast augmentation is tremendous help to patients who desire a fuller profile, who have lost breast volume due to pregnancy or nursing, or who have undergone breast reconstruction and want to gain a more natural look again.
Chronic obstructive pulmonary disease (COPD) is defined as progressive, chronic airflow obstruction due to chronic bronchitis, emphysema, or both. The majority of patients have components of both, although one of these entities will frequently dominate the clinical picture. Emphysema�airspace enlargement distal to the terminal bronchioles due to destruction of alveolar septa. Chronic bronchitis�chronic airway inflammation and bronchospasm. Clinically defined as productive cough lasting for at least 3 mo over 2 consecutive years. Although COPD is irreversible, patients with acute exacerbations do have reversible bronchospastic and inflammatory components.

reast Augmentation: From Cost to Complications || Common gynaecological problems in women Breast augmentation (aka augmentation mammaplasty) is one of the most popular cosmetic procedures performed in the U.S. today. Despite controversy over the use of silicone breast implants, women have shown a continuing and growing eagerness to surgically enhance the size and shape of their breasts. If you are a healthy, non-smoking women who are at or near their ideal weight, with enough of their own breast tissue to cover and support an implant adequately, then you are a good candidate for breast augmentation surgery.
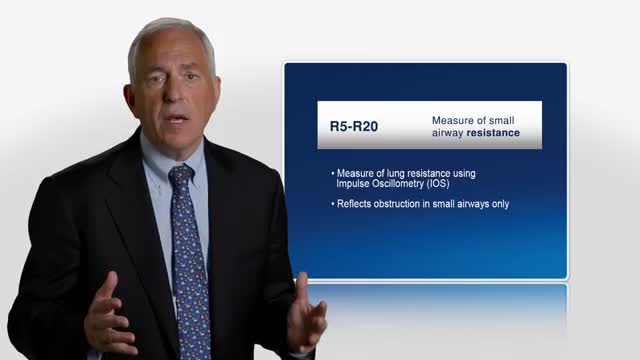
Asthma was originally described as an inflammatory disease that predominantly involves the central airways. Pathological and physiological evidence reported during the past few years suggests that the inflammatory process extends beyond the central airways to the peripheral airways and the lung parenchyma. The small airways are capable of producing T-helper-2 cytokines, as well as chemokines, and they have recently been recognized as a predominant site of airflow obstruction in asthmatic persons. The inflammation at this distal site has been described as more severe than large airway inflammation. These findings are of great clinical significance, and highlight the need to consider the peripheral airways as a target in any therapeutic strategy for treatment of asthma.

