- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
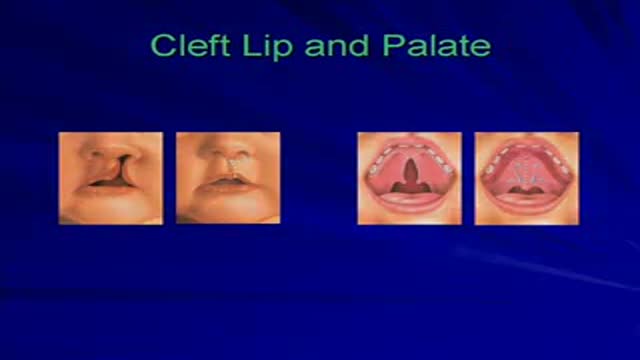
This video is a collection of selected cases of Plastic Surgery performed on children with congenital deformities.
Errata: Cleft Lip Case 2 has a center photo which belongs to case 1 at day of surgery.

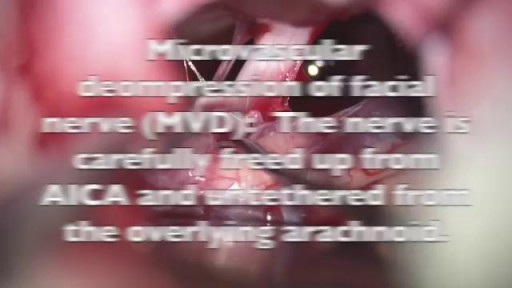
This video shows a surgery of Brain Microvascular Decompression of facial nerve for hemifacial spasm

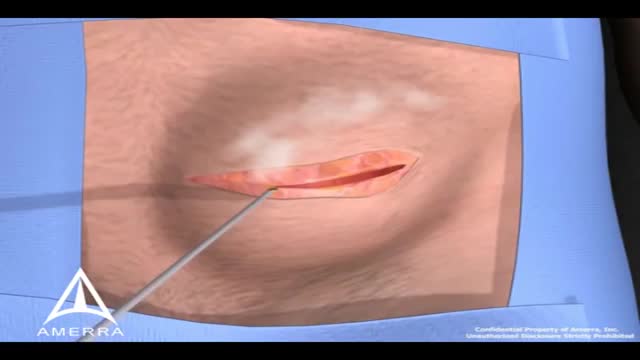
A nonsurgical method of treating a ganglion is to drain the fluid from (aspirate) the ganglion sac. Your doctor can do this in the office using the following procedure: The ganglion area is cleaned with an antiseptic solution. A local anesthetic is injected into the ganglion area to numb the area. When the area is numb, the ganglion sac is punctured with a sterile needle. The fluid is drawn out of the ganglion sac. The ganglion collapses. A bandage and, in some cases, a splint are used for a few days to limit movement and prevent the ganglion sac from filling again. Treating a ganglion by draining the fluid with a needle may not work because the ganglion sac remains intact and can fill again, causing the ganglion to return. For this reason, your doctor may puncture the sac with the needle 3 or 4 times so the sac will collapse completely. Even then, the ganglion is likely to come back.

What is hemodiafiltration? Hemodiafiltration, or HDF, is a renal replacement modality that combines diffusion and convection to improve removal of molecules in the middle molecular weight range versus hemodialysis.
Find our full video library only on Osmosis Prime: http://osms.it/more.
Join over 3 million current & future clinicians who learn by Osmosis, and over 130 universities around the world who partner with us to make medical and health education more engaging and efficient. We have unparalleled tools and materials to prepare you to succeed in school, on board exams, and as a future clinician. Sign up for a free trial at http://osms.it/more. If you're interested in exploring an institutional partnership, visit osmosis.org/educators to request a personalized demo.
Follow us on social:
Facebook: http://osms.it/facebook
Twitter: http://osms.it/twitter
Instagram for med: http://osms.it/instagram
Instagram for nursing: https://osms.it/ignursing
Linkedin: https://osms.it/linkedin
Our Vision: Everyone who cares for someone will learn by Osmosis.
Our Mission: To empower the world’s clinicians and caregivers with the best learning experience possible. Learn more here: http://osms.it/mission
Medical disclaimer: Knowledge Diffusion Inc (DBA Osmosis) does not provide medical advice. Osmosis and the content available on Osmosis's properties (Osmosis.org, YouTube, and other channels) do not provide a diagnosis or other recommendation for treatment and are not a substitute for the professional judgment of a healthcare professional in diagnosis and treatment of any person or animal. The determination of the need for medical services and the types of healthcare to be provided to a patient are decisions that should be made only by a physician or other licensed health care provider. Always seek the advice of a physician or other qualified healthcare provider with any questions you have regarding a medical condition. © 2023 Elsevier. All rights reserved.
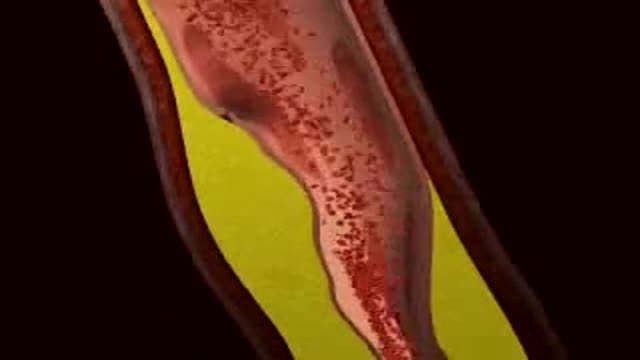
Myocardial Infarction 3D Animation

Special Anoscope for Easy Purse string Suture Application in Stapled Hemorrhoidopexy

Mode of action of NNRTIs

Watch that video to know What Causes Trypophobia?
During surgery to repair the hernia, the bulging tissue is pushed back in. Your abdominal wall is strengthened and supported with sutures (stitches), and sometimes mesh. This repair can be done with open or laparoscopic surgery. You and your surgeon can discuss which type of surgery is right for you.
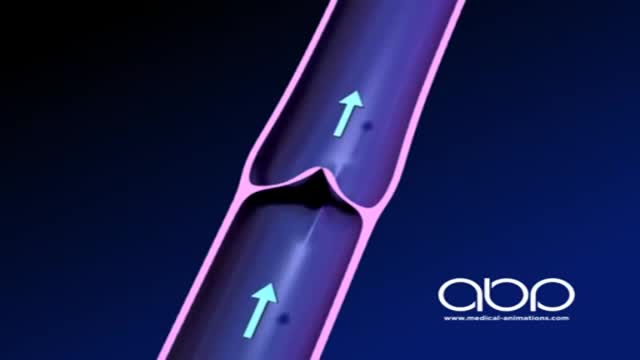
The deep veins play a significant role in propelling blood toward the heart. The one-way valves in deep veins prevent blood from flowing backward, and the muscles surrounding the deep veins compress them, helping force the blood toward the heart, just as squeezing a toothpaste tube ejects toothpaste.

Natural birth encouragement pain and joy

A wisdom tooth or third molar is one of the three molars per quadrant of the human dentition. It is the most posterior of the three. Wisdom teeth generally erupt between the ages of 17

Today I will discuss about hemodialysis.
Start with a free 3-day trial at ReMarNurse.com/FREE
Follow & Subscribe for more weekly nursing and NCLEX content every Monday and Wednesday with Regina MSN, RN!
00:00 Introduction
02:53 Hemodialysis
06:06 Dialysis Apparatus
07:59 Dialysis Mechanism
13:27 Vascular Access
18:55 Nursing Considerations
25:07 Nursing Management for HD
27:57 NCLEX Practice Questions
Hemodialysis is a procedure where a dialysis machine and a special filter called an artificial kidney, or a dialyzer, are used to clean your blood.
I will also discuss about hemodialysis procedure, how hemodialysis machine works and its benefits for patients.
If you're interested in learning more about hemodialysis, or if this just seems like something you should know for nursing school or for the NCLEX exam, check out this video!
Join the #1 community of nursing students on the planet with 12,000+ students studying now inside of the NCLEX Virtual Trainer review on sale now at http://www.ReMarNurse.com
► Subscribe to JOIN the ReMar YouTube Channel: http://bit.ly/ReMar-Subscription
Your NCLEX RN & LPN Study Tools:
► Get NCLEX Virtual Trainer: http://www.ReMarNurse.com/NCLEXVT
► Get the Question Bank: http://www.ReMarNurse.com/NCLEXQBank
► Get Quick Facts for NCLEX: http://bit.ly/QuickFactsNCLEX
Get MORE from Regina MSN, RN:
► WATCH MORE: http://bit.ly/PassNCLEXPlayList/
► GET THE PODCAST: https://remarnurse.podbean.com/
► WATCH LESSONS: http://bit.ly/ReMarNCLEXLectures/
► FOLLOW ReMar on Instagram: https://www.instagram.com/ReMarNurse/
► LIKE ReMar on Facebook: https://www.facebook.com/ReMarReview/
#nursingstudent #hemodialysis #nursing #remarreview
ReMar Review features weekly NCLEX review questions and lectures from Regina M. Callion MSN, RN. ReMar is the #1 content-based NCLEX review and has helped thousands of repeat-testers pass NCLEX with a 99.2% student success rate!
ReMar focuses on 100% core nursing content and as a result, has the best review to help nursing students pass boards - fast!
Hepatitis and chronic alcohol abuse are frequent causes. Liver damage caused by cirrhosis can't be undone, but further damage can be limited. Initially patients may experience fatigue, weakness, and weight loss. During later stages, patients may develop jaundice (yellowing of the skin), gastrointestinal bleeding, abdominal swelling, and confusion. Treatments focus on the underlying cause. In advanced cases, a liver transplant may be needed.
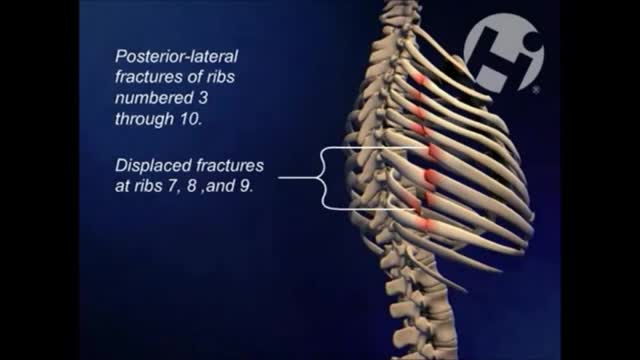
hemothorax is most often defined as rapid accumulation of ≥ 1000 mL of blood. Shock is common. Patients with large hemorrhage volume are often dyspneic and have decreased breath sounds and dullness to percussion (often difficult to appreciate during initial evaluation of patients with multiple injuries).

Watch that video of the 10 Most Invasive Parasites in the World
Lysosomal storage diseases (LSDs; /ˌlaɪsəˈsoʊməl/) are a group of approximately 50 rare inherited metabolic disorders that result from defects in lysosomal function. Lysosomes are sacs of enzymes within cells that digest large molecules and pass the fragments on to other parts of the cell for recycling.

Medical Terminology
