トップ動画
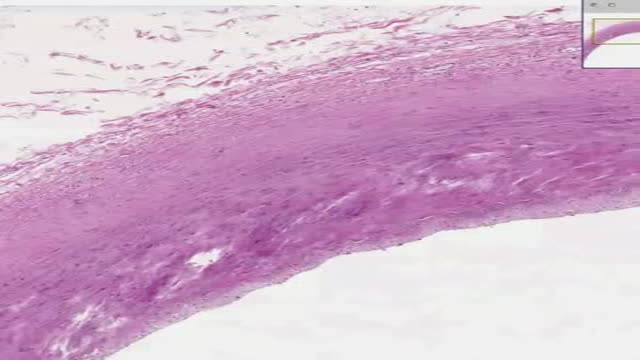
Histology of Large Artery

Most people develop several moles (nevi) throughout adulthood. Moles can be found anywhere on the body, usually in sun-exposed areas, and are usually brown, smooth, and slightly raised. In most cases, a nevus is benign and doesn't require treatment. Rarely, they turn into melanoma or other skin cancers. A nevus that changes shape, grows bigger, or darkens should be evaluated for removal.
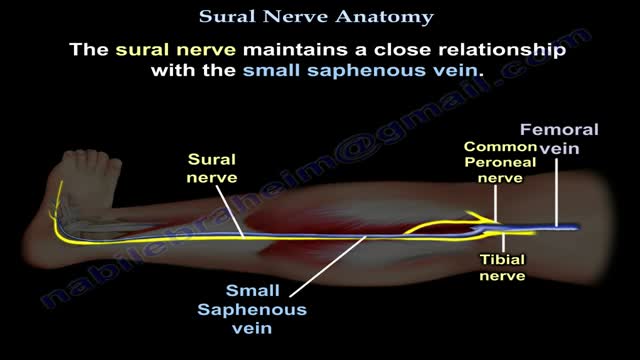
Nerves are the organs that make up the peripheral nervous system (PNS). They serve as information pipelines that allow the brain and spinal cord to communicate with other tissues and organs. Inside the nerves are the axon processes of sensory and motor neurons (nerve cells).
Wound healing is the process by which skin or other body tissue repairs itself after trauma. ... This process is divided into predictable phases: blood clotting (hemostasis), inflammation, tissue growth (proliferation) and tissue remodeling (maturation).
The accumulation of ascitic fluid represents a state of total-body sodium and water excess, but the event that initiates the unbalance is unclear. Although many pathogenic processes have been implicated in the development of abdominal ascites, about 75% likely occur as a result of portal hypertension in the setting of liver cirrhosis, with the remainder due to infective, inflammatory, and infiltrative conditions. Three theories of ascites formation have been proposed: underfilling, overflow, and peripheral arterial vasodilation. The underfilling theory suggests that the primary abnormality is inappropriate sequestration of fluid within the splanchnic vascular bed due to portal hypertension and a consequent decrease in effective circulating blood volume. This activates the plasma renin, aldosterone, and sympathetic nervous system, resulting in renal sodium and water retention. The overflow theory suggests that the primary abnormality is inappropriate renal retention of sodium and water in the absence of volume depletion. This theory was developed in accordance with the observation that patients with cirrhosis have intravascular hypervolemia rather than hypovolemia. The most recent theory, the peripheral arterial vasodilation hypothesis, includes components of both of the other theories. It suggests that portal hypertension leads to vasodilation, which causes decreased effective arterial blood volume. As the natural history of the disease progresses, neurohumoral excitation increases, more renal sodium is retained, and plasma volume expands. This leads to overflow of fluid into the peritoneal cavity. The vasodilation theory proposes that underfilling is operative early and overflow is operative late in the natural history of cirrhosis. Although the sequence of events that occurs between the development of portal hypertension and renal sodium retention is not entirely clear, portal hypertension apparently leads to an increase in nitric oxide levels. Nitric oxide mediates splanchnic and peripheral vasodilation. Hepatic artery nitric oxide synthase activity is greater in patients with ascites than in those without ascites. Regardless of the initiating event, a number of factors contribute to the accumulation of fluid in the abdominal cavity. Elevated levels of epinephrine and norepinephrine are well-documented factors. Hypoalbuminemia and reduced plasma oncotic pressure favor the extravasation of fluid from the plasma to the peritoneal fluid, and, thus, ascites is infrequent in patients with cirrhosis unless both portal hypertension and hypoalbuminemia are present.
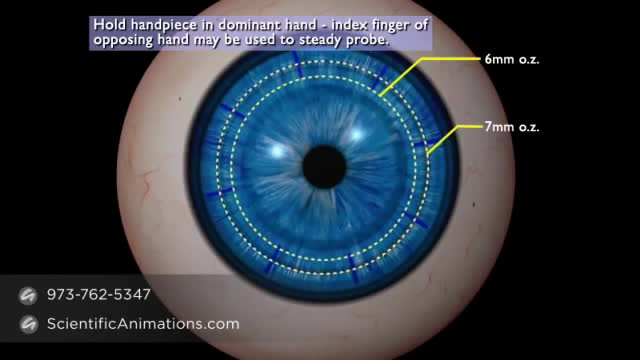
Keratoplasty is the procedure whereby abnormal corneal tissue is replaced by a healthy donor cornea.

Laser- Removal of Salivary Stone


Watch that video of the 10 Most Invasive Parasites in the World
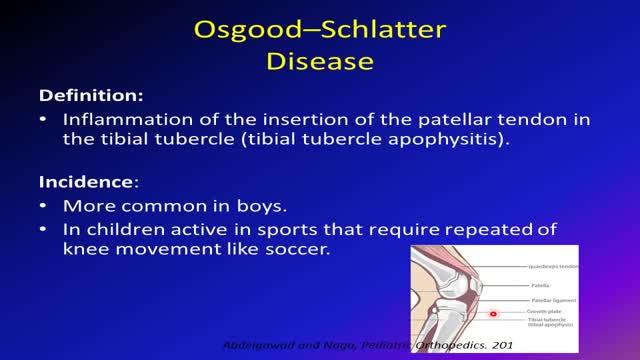
Osgood-Schlatter disease can cause a painful lump below the kneecap in children and adolescents experiencing growth spurts during puberty. Osgood-Schlatter disease occurs most often in children who participate in sports that involve running, jumping and swift changes of direction — such as soccer, basketball, figure skating and ballet. While Osgood-Schlatter disease is more common in boys, the gender gap is narrowing as more girls become involved with sports. Age ranges differ by sex because girls experience puberty earlier than do boys. Osgood-Schlatter disease typically occurs in boys ages 13 to 14 and girls ages 11 to 12. The condition usually resolves on its own, once the child's bones stop growing.

You're sneezing, coughing, and all stuffed up. It sounds and feels like a cold, alright. But as time goes on, you start to wonder. Is it turning into a sinus infection? They've got some things in common, but there are ways to tell them apart. The right ID lets your doctor get you the best treatment. What Is a Common Cold? It's an infection caused by a virus, a tiny living thing. You can't miss the symptoms: Nasal congestion Runny nose Post-nasal drip (drop-by-drop release of fluid from your nose into the back of the throat) Headache Fatigue You may also get a cough and a mild fever. The symptoms usually build, peak, and slowly disappear. Some medications can ease symptoms. For example, decongestants may decrease drainage and open the nasal passages. Pain relievers may help with fever and headache. Cough medicine may help, as well. Colds typically last from a few days to about a week or longer. Sometimes, a cold may cause swelling in the sinuses, hollow spaces in your skull that are connected to each other. The swelling can prevent the flow of mucus.

New Treatment for sinusitis. Yamik procedure

Mini-Laparoscopic Cholecystectomy with Intraoperative Cholangiogram for Symptomatic Cholelithiasis (Gallstones) - Standard
Authors: Brunt LM1, Singh R1, Yee A2
Published: September 26, 2017
AUTHOR INFORMATION
1 Department of Surgery, Washington University, St. Louis, Missouri
2 Division of Plastic and Reconstructive Surgery, Washington University, St. Louis, Missouri
DISCLOSURE
No authors have a financial interest in any of the products, devices, or drugs mentioned in this production or publication.
ABSTRACT
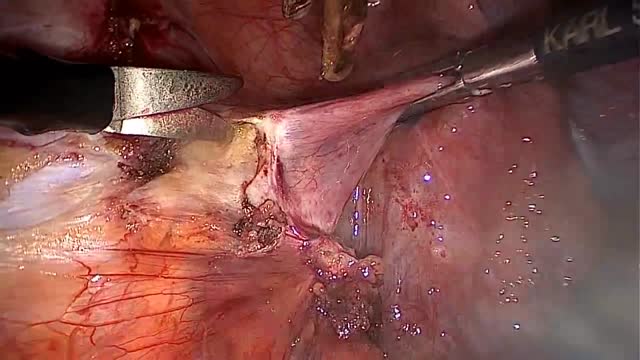
Minimal invasive laparoscopic cholecystectomy is the typical surgical treatment for cholelithiasis (gallstones), where patients present with a history of upper abdominal pain and episodes of biliary colic. The classic technique for minimal invasive laparoscopic cholecystectomy involves four ports: one umbilicus port, two subcostal ports, and a single epigastric port. The Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) has instituted a six-step strategy to foster a universal culture of safety for cholecystectomy and minimize risk of bile duct injury. The technical steps are documented within the context of the surgical video for (1) achieving a critical view of safety for identification of the cystic duct and artery, (2) intraoperative time-out prior to management of the ductal structures, (3) recognizing the zone of significant risk of injury, and (4) routine intraoperative cholangiography for imaging of the biliary tree. In this case, the patient presented with symptomatic biliary colic due to a gallstone seen on the ultrasound in the gallbladder. The patient was managed a mini-laparoscopic cholecystectomy using 3mm ports for the epigastric and subcostal port sites with intraoperative fluoroscopic cholangiogram. Specifically, the senior author encountered a tight cystic duct preventing the insertion of the cholangiocatheter and the surgical video describes how the author managed the cystic duct for achieving a cholangiogram, in addition to the entire technical details of laparoscopic cholecystectomy.
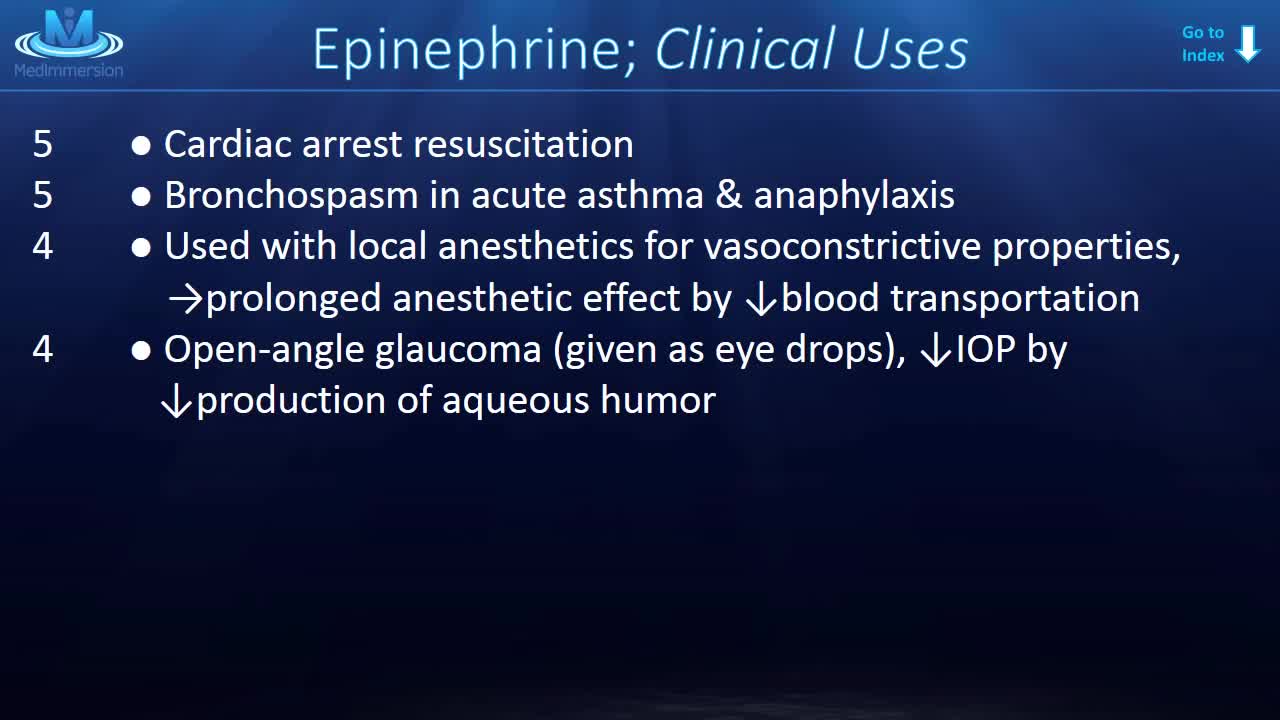
This medication is used in emergencies to treat very serious allergic reactions to insect stings/bites, foods, drugs, or other substances. Epinephrine acts quickly to improve breathing, stimulate the heart, raise a dropping blood pressure, reverse hives, and reduce swelling of the face, lips, and throat.
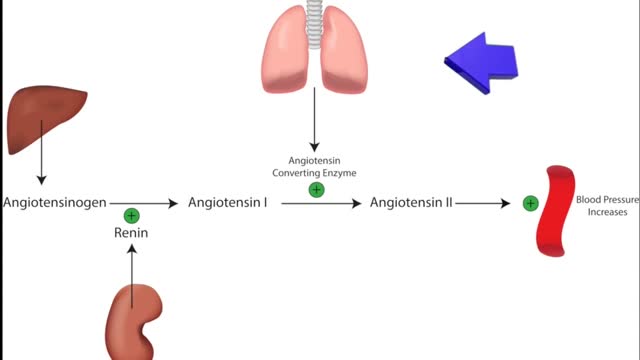
ACE inhibitors Email this page to a friend Print Facebook Twitter Google+ Angiotensin-converting enzyme (ACE) inhibitors are medicines. They treat heart, blood vessel, and kidney problems. How ACE inhibitors help ACE inhibitors are used to treat heart disease. These medicines make your heart work less hard by lowering your blood pressure. This keeps some kinds of heart disease from getting worse. Most people who have heart failure take these medicines. These medicines treat high blood pressure, strokes, or heart attacks. They may help lower your risk for stroke or heart attack. They are also used to treat diabetes and kidney problems. This can help keep your kidneys from getting worse. If you have these problems, ask your health care provider if you should be taking these medicines.
LAPAROSCOPIC END TO END URETERAL ANASTOMOSIS
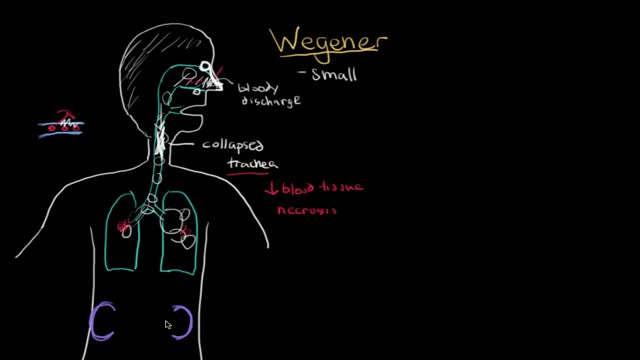
Microscopic polyangiitis (MPA) is vasculitis of small vessels. It was initially considered as a microscopic form of polyarteritis nodosa (PAN). In 1990, the American College of Rheumatology developed classification criteria for several types of systemic vasculitis but did not distinguish between polyarteritis nodosa and microscopic polyarteritis nodosa. [1] In 1994, a group of experts held an international consensus conference in Chapel Hill, North Carolina, to attempt to redefine the classification of small vessel vasculitides. [2, 3]
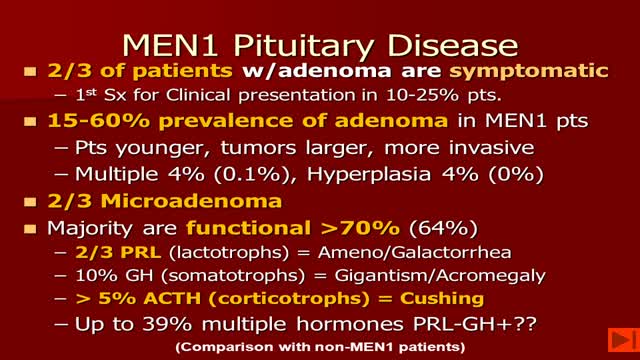
-MEN1 syndrome is composed of hyperparathyroidism, gastrinoma (pancreatic tumor) and pituitary tum or(remember the 3 Ps). Hyperparathyroidism in MEN1 is caused by hyperplasia of the parathyroid glands. Removal of 3 1/2 glands or total parathyroidectomy with autotransplantation is necessary.
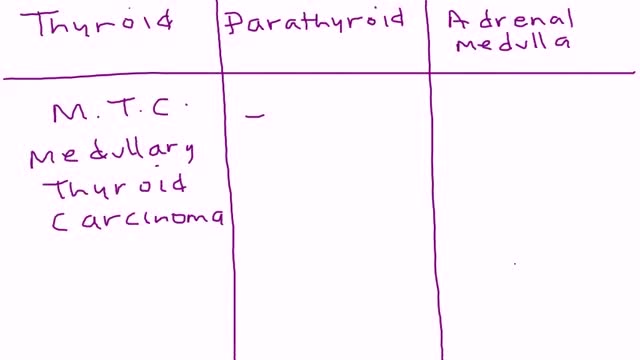
Multiple endocrine neoplasia type 2 (MEN2) (also known as "Pheochromocytoma and amyloid producing medullary thyroid carcinoma", "PTC syndrome," and "Sipple syndrome") is a group of medical disorders associated with tumors of the endocrine system. The tumors may be benign or malignant (cancer).

We will show how to know if you have a sports hernia. These are a few tests you can do on your own. Lower abdominal pain and tightness that increases with twisting and kicking. Stretching and exercises tend to make the discomfort increase.
Want more info? We have a free webinar that covers hip, groin, adductor, lower abdominal strains and sports hernia diagnosis in detail. Use this link to get access. https://bit.ly/37thtNF
#sportshernia #hernia #hippain
To work with us, contact us using this link https://bit.ly/3zCBnzZ or call us 714-502-4243. We have online programs, virtual and in-person options.
Costa Mesa, CA www.p2sportscare.com
Option 1: Groin On-Demand Webinar https://bit.ly/37thtNF
Option 2: Video Guide https://bit.ly/33aLIqC
Option 3 (the best): Work With Us https://www.p2sportscare.com/
Sports Hernia Diagnosis
What Is A Sports Hernia?
A sports hernia is tearing of the transversalis fascia of the lower abdominal or groin region. A common misconception is that a sports hernia is the same as a traditional hernia. The mechanism of injury is rapid twisting and change of direction within sports, such as football, basketball, soccer and hockey.
The term “sports hernia” is becoming mainstream with more professional athletes being diagnosed. The following are just to name a few:
Torii Hunter
Tom Brady
Ryan Getzlaf
Julio Jones
Jeremy Shockey
If you follow any of these professional athletes, they all seem to have the same thing in common: Lingering groin pain. If you play fantasy sports, this is a major headache since it seems so minor, but it can land a player on Injury Reserve on a moments notice. In real life, it is a very frustrating condition to say the least. It is hard to pin point, goes away with rest and comes back after activity, but is hardly painful enough to make you want to stop. It lingers and is always on your mind. And if you’re looking for my step-by-step sports hernia rehab video course here it is.
One the best definitions of Sport hernias is the following by Harmon:
The phenomena of chronic activity–related groin pain that it is unresponsive to conservative therapy and significantly improves with surgical repair.”
This is truly how sports hernias behave in a clinical setting. It is not uncommon for a sports hernia to be unrecognized for months and even years. Unlike your typical sports injury, most sports medicine offices have only seen a handful of cases. It’s just not on most doctors’ radar. The purpose of this article is not only to bring awareness about sports hernias, but also to educate.
Will you find quick fixes in this article for sports hernia rehab?
Nope. There is no quick fix for this condition, and if someone is trying to sell you one, they are blowing smoke up your you-know-what.
Is there a way to decrease the pain related to sports hernias?
Yes. Proper rehab and avoidance of activity for a certain period of time will assist greatly, but this will not always stop it from coming back. Pain is the first thing to go and last thing to come. Do not be fooled when you become pain-free by resting it. Pain is only one measure of improvement in your rehab. Strength, change of direction, balance and power (just to name a few) are important, since you obviously desire to play your sport again. If you wanted to be a couch potato, you would be feeling better in no time. Watching Sports Center doesn’t require any movement.
Why is this article so long?
There is a lot of information on sports hernias available to you on the web. However, much of the information is spread out all over the internet and hard for athletes to digest due to complicated terminology. This article lays out the foundational terminology you will need to understand what options you have with your injury. We will go over anatomy, biomechanics, rehab, surgery, and even the fun facts. The information I am using is from the last ten years of medical research, up until 2016. We will be making updates overtime when something new is found as well. So link to this page and share with friends. This is the best source for information on sports hernias you will find.
Common Names (or Aliases?) for Sports Hernias
Sportsman’s Hernia
Athletic Pubalgia
Gilmore’s Groin
How Do You Know If You Have A Sports Hernia?
Typical athlete characteristics:
Male, age mid-20s
Common sports: soccer, hockey, tennis, football, field hockey
Motions involved: cutting, pivoting, kicking and sharp turns
Gradual onset
How A Sports Hernia Develops
Chronic groin pain typically happens over time, which is why with sports hernias, we do not hear many stories of feeling a “pop” or a specific moment of injury. It is the result of “overuse” mechanics stemming from a combination of inadequate strength and endurance, lack of dynamic control, movement pattern abnormalities, and discoordination of motion in the groin area.
