- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
How To Stop Hair Loss Naturally, Hair Regrowth Shampoo, Tips For Hair Regrowth, Hair Loss Stop--- http://how-to-regrow-your-hair.info-pro.co/ --- Natural Hair Regrowth Treatment, Looking for ideas on natural hair regrowth treatment? There are actually a lot of safe and effective natural methods that you can try in order to reverse hair loss. So what are those natural methods? Here are some of them: Eat your way to better hair: Hard to believe isn’t it? To think that what you’re actually eating can affect your hair in so many ways, positively and negatively. Want to slow down the process of hair loss and get your hair back to the healthy original state you always remembered it in? Then you might want to start transitioning over to a low fat high fiber diet. Aside from this, you’ll also want to concentrate on foods that contain biotins, which play an essential role in maintaining healthy hair. Fish, cooked eggs, whole milk, and various nuts and fruits – all of these are good sources of biotins so it’s best that you take note of them. Drink plenty of water: It’s not only that gets thirsty, as even your hair requires the moisture that water provides. Dehydration can lead to symptoms like constipation, eczema, thick dandruff, wrinkly skin, foul breath and hair loss. Remember that your body is made up of 98% water and you need to maintain it at optimum levels if you want to keep your hair in place. An easy way to quickly replenish and establish enough water in your body is to routinely drink at least 8 ounces of water immediately after you urinate. You’ll know you’re getting enough water when you observe that you are urinating more frequently. Supplements: The fact that you are experiencing hair loss is a surefire indication that something is amiss in the nutrition department. If you are however looking for a definitive guide on the products that will be available, one useful source you can use will be found at http://how-to-regrow-your-hair.info-pro.co/

allux valgus is considered to involve the following: Medial deviation of the first metatarsal Lateral deviation and/or rotation of the hallux Prominence, with or without medial soft-tissue enlargement of the first metatarsal head

💥Patellar Tendon Pain AKA “Jumper’s Knee”👇
💥If you have this, it’s likely because your patellar tendon was over-stressed beyond what it can currently handle (due to loads that are too high or lack of recovery).
🔑 Try 5 reps of 45 second holds
🔑 2 min of rest in between each rep
🔑 Keep your knees at roughly 60 deg angle
🔑 7/10 intensity
🔑Should not increase pain during or after exercise
📚A research article found that this protocol using a knee extension machine provided significant short term pain relief. Most people don’t have a knee extension machine at home, so you could try out a wall sit instead!
🔑It may be useful during the season of competition to decrease pain and allow the athlete to compete, if needed.
❤️ Share this video with a friend who needs it!
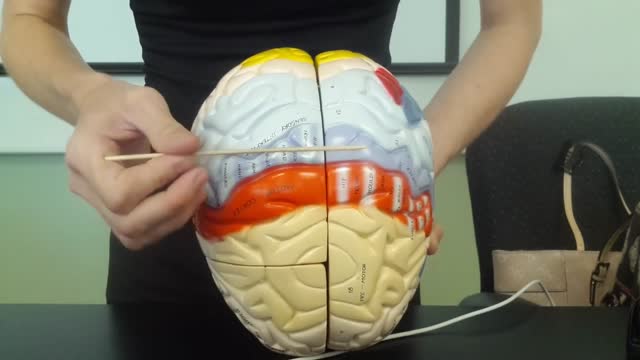
The brain is that part of the CNS contained within the cranial cavity (figure 13.1). It is the control center for many of the body's functions. The brain is much like a complex central computer but with additional functions that no computer can as yet match. Indeed, one goal in computer technology is to make computers that can function more like the human brain. The brain consists of the brainstem, the cerebellum, the diencephalon, and the cerebrum (table 13.1). The brainstem includes the medulla oblongata, pons, midbrain, and reticular formation. The structure of the brain is described in this chapter. Its functions are primarily discussed in chapter 14. Twelve pairs of cranial nerves, which are part of the PNS, arise directly from the brain. Two pairs arise from the cerebrum, nine pairs arise from the brainstem, and one pair arises from the spinal cord.

A simple continuous stitch can be a useful technique for skin closure when speed is important, e.g. closing a scalp laceration on a screaming child. The simple running, or continuous suture, is begun in the same way as a simple interrupted suture.
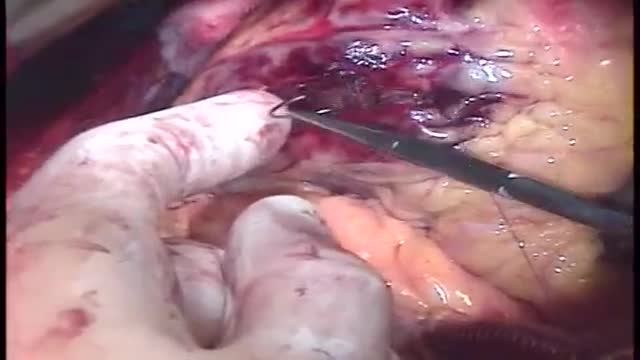
Repair of post-infarction ventricular septal defect (VSD) remains a challenging procedure with a high risk of VSD recurrence. In order to reduce this risk, a double patch and glue technique was introduced in the department in 1986. This surgical technique is hereunder presented. Since 1971, ninety-three patients have been operated on early (≪15 days) after the occurrence of a post-infarction VSD. This retrospective study allows to compare the results of this double patch and glue technique to those obtained with the conventional one, in terms of hospital death and VSD recurrence. The double patch and glue technique avoids recurrence of VSD and plays a part in reducing hospital mortality.

The majority of epileptic seizures are controlled by medication, particularly anticonvulsant drugs. The type of treatment prescribed will depend on several factors, including the frequency and severity of the seizures and the person's age, overall health, and medical history. An accurate diagnosis of the type of epilepsy is also critical to choosing the best treatment. Drug Therapy Many drugs are available to treat epilepsy. Although generic drugs are safely used for most medications, anticonvulsants are one category where doctors proceed with caution. Most doctors prefer to use brand-name anticonvulsants, but realize that many insurance companies will not cover the cost. As a result, it is acceptable to start taking a generic anticonvulsant medication, but if the desired control is not achieved, the patient should be switched to the brand-name drug.
There's only one group of people who really know what happens when you die: the dead. And since the dead won't be revealing their secrets anytime soon, it's up to scientists to explain what happens when a person dies. Death, just like life, is a process, scientists say. The first stage of this process is known as clinical death. It lasts from four to six minutes, beginning when a person stops breathing and the heart stops pumping blood. During this time, there may be enough oxygen in the brain that no permanent brain damage occurs. Other organs, such as the kidneys and eyes, also remain alive throughout clinical death.
Bovine respiratory disease (BRD) has a multifactorial etiology and develops as a result of complex interactions between environmental factors, host factors, and pathogens. Environmental factors (eg, weaning, transport, commingling, crowding, inclement weather, dust, and inadequate ventilation) serve as stressors that adversely affect the immune and nonimmune defense mechanisms of the host. In addition, certain environmental factors (eg, crowding and inadequate ventilation) can enhance the transmission of infectious agents among animals. Many infectious agents have been associated with BRD. An initial pathogen (eg, a virus) may alter the animal’s defense mechanisms, allowing colonization of the lower respiratory tract by bacteria.

You get motion sickness when one part of your balance-sensing system (your inner ear , eyes, and sensory nerves) senses that your body is moving, but the other parts don't. For example, if you are in the cabin of a moving ship, your inner ear may sense the motion of waves, but your eyes don't see any movement.

A pneumothorax is usually caused by an injury to the chest, such as a broken rib or puncture wound. It may also occur suddenly without an injury. A pneumothorax can result from damage to the lungs caused by conditions such as chronic obstructive pulmonary disease (COPD), asthma, cystic fibrosis, and pneumonia.

irregular, curved toenails. footwear that places a lot of pressure on the big toes, such as socks and stockings that are too tight or shoes that are too tight, narrow, or flat for your feet. toenail injury, including stubbing your toe, dropping something heavy on your foot, or kicking a ball repeatedly. poor posture.

Adult-onset Still's disease (AOSD) is a rare systemic inflammatory disease characterized by the classic triad of persistent high spiking fevers, joint pain, and a distinctive salmon-colored bumpy rash. The disease is considered a diagnosis of exclusion.

Smoking causes: Chronic obstructive pulmonary disease (COPD), a disease that gets worse over time and causes wheezing, shortness of breath, chest tightness, and other symptoms. Emphysema, a condition in which the walls between the air sacs in your lungs lose their ability to stretch and shrink back.
Trisomy 18, also called Edwards syndrome, is a chromosomal condition associated with abnormalities in many parts of the body. Individuals with trisomy 18 often have slow growth before birth (intrauterine growth retardation) and a low birth weight. Affected individuals may have heart defects and abnormalities of other organs that develop before birth. Other features of trisomy 18 include a small, abnormally shaped head; a small jaw and mouth; and clenched fists with overlapping fingers. Due to the presence of several life-threatening medical problems, many individuals with trisomy 18 die before birth or within their first month. Five to 10 percent of children with this condition live past their first year, and these children often have severe intellectual disability.

Endometriosis (en-doe-me-tree-O-sis) is an often painful disorder in which tissue that normally lines the inside of your uterus — the endometrium — grows outside your uterus. Endometriosis most commonly involves your ovaries, fallopian tubes and the tissue lining your pelvis. Rarely, endometrial tissue may spread beyond pelvic organs.
Adrenoleukodystrophy, or ALD, is a deadly genetic disease that affects 1 in 18 000 people. It most severely affects boys and men. This brain disorder destroys myelin, the protective sheath that surrounds the brain's neurons -- the nerve cells that allow us to think and to control our muscles.
A hemolytic transfusion reaction is a serious complication that can occur after a transfusion of blood. The red blood cells that were given in the transfusion are destroyed by the patient's immune system. There are other types of allergic transfusion reactions that do not cause hemolysis.
Vertebrobasilar insufficiency is typically secondary to emboli, thrombi, or arterial dissection. The labyrinth and brainstem are commonly affected, and symptoms may include vertigo, dizziness, dysarthria, diplopia, and numbness.
CD4 T-cells (a type of white blood cell) are important to your body's defence against infections. This animation describes how your immune system is weakened by the HIV virus, which targets CD4 T-cells and leads to their gradual decline in number. Low to very low levels of CD4 cells put you at risk for 'opportunistic infections' that take advantage of the body's weakened immune system.
