- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Watch that video of a Snake bite causes girl’s leg to rot away

hemisplenectomy is removal of the half of the spleen.It was done firstly in Azerbaijan by prof. Dr Med Qurban Muslimov in 12 years old child with simple syst of the spleen.

Tuberous breast deformity is a congenital breast anomaly that becomes manifest at the time of puberty and breast development. The three components of tubular deformity usually include, pseudoherniation of breast tissue into the nipple areolar complex, poorly defined inframammary fold and flattening of the lower pole of the breast which leads to a conical tubular shape. Stuart Linder M.D. 9675 BRIGHTON WAY, SUITE 420 BEVERLY HILLS CA 90210 (310) 275-4513

Once the diagnosis of a splenic abscess has been made, the patient must be admitted to the hospital and treated. Treatment depends on the patient's overall condition, comorbidities, and primary disorder (if any), as well as the size and topography of the abscess
Tension pneumothorax describes the progressive accumulation of air in the pleural cavity (normally a potential space) through a defect in the visceral pleura. This leads to positive pressure being maintained and increasing throughout the respiratory cycle causing vessels within the mediastinum to be compressed with catastrophic consequences if left untreated. Clinical signs include hypoxia, hypotension, tachycardia, reduced breath sounds and hyper resonance ipsilaterally, with tracheal deviation (away from the affected side) and distended neck veins being late clinical signs.

Do you think you have a hernia?
What are hernias?
The hernias we address in this http://DoctorsExpressHartsdale.com Medical Minute are inguinal, or groin, hernias. More common in men than women, an inguinal hernia can occur when part of the small intestine protrudes through a weakness or tear in the area between your abdomen and your thigh- or your groin. It's possible for anyone to get an inguinal hernia, but it is more commonly found in males.
Hernias form a bulge and can be accompanied by pain. Men have an approximate 26% lifetime risk of having hernia at some point in their life, where as women have a much lower chance of one- only about 3% of women will experience a hernia at some point in their life. There are other types of hernias, such as abdominal, or "hiatal" hernias but groin hernias outnumber abdominal hernias by about 3 to 1.
What causes a hernia?
The cause of a hernia is not always known, but hernias are often the result of weak spots in the abdominal wall. Weaknesses can be due to congenital defects (present at birth) or formed later in life. Some risk factors for inguinal hernia include:
• fluid or pressure in the abdomen
• heavy lifting
• straining during urination or bowel movements
• obesity
• chronic cough
• pregnancy
Hernias often form in people with weakened abdominal muscles or in those who do a lot of heavy lifting or straining, which is why we see it quite often in young men. Physiology plays a part: men have testicles and scrotum which descend through the inguinal canal-much larger in men than in women. That is part of the reason men tend to be more susceptible to hernias than women.
Symptoms of hernia
Symptoms of inguinal hernia usually include a bulge in the groin area and pain, pressure, or aching at the bulge—especially when lifting, bending, or coughing. These symptoms usually subside during rest periods. Men may also experience swelling around the testicles.
Screening and Diagnosis of Hernias
If you are having abdominal pain or pelvic bulge and pain, you want to see physician, and he or she will do an exam. They will use their finger, to see if you have a bulge in your scrotum or on your groin and they'll see if its reducible or not. If the exam doesn't give them the answer, they can then perform an ultrasound, an inexpensive test that can tell you the same day whether a hernia is present.
What to do if you think you have a hernia
Most of the time hernias do not cause problems. People often live with hernias their entire life without them becoming aggravated or painful. When they do cause pain though, there is concern that complications may have arisen. Most common hernias are what we call reducible; you can take your finger or you can lie down in bed and due to the effects of gravity, the bulge in the groin will actually disappear, which means the intestinal contents actually go back into the abdominal cavity or to the correct location. If it's not reducible by lying down or using a finger or having a physician trying to reduce it, then there are concerns about complications such as strangulation, or incarceration occurring. If those concerns are there, then you need to see a surgeon, and there may be a need for surgery.
How to Treat a Hernia
As stated earlier, hernias can often be watched for years without being treated. If however, they are causing pain, we generally refer you to a surgeon who can do a very simple laparoscopic surgery.
If you suspect a hernia, but have not been diagnosed, you should see your doctor, and of course, we are happy to see you here at Doctors Express

Achieving and maintaining long-term weight loss goals.

Today, the most common approach for open-heart surgery is a sternotomy, which requires a 12-14-inch incision through the breastbone. But in the hands of experienced minimally invasive surgeons, many cardiac procedures can be performed through smaller 2- to 3-inch incisions between the ribs without the need to cut through the breastbone. Learn more in this medical animation from Sarasota Memorial's Minimally Invasive Cardiac Surgery Team and medical director Jonathan Hoffberger, DO. For information or referrals, visit smhheart.com.

Hydatid cysts in retroperitoneal region in transit to the thorax

This 3D medical animation shows several methods of breast tissue biopsy procedures including:
- Needle biopsy,
- Stereotactic core biopsy
- Ultrasound-guided core biopsy - - Surgical biopsy
Endoscopy of Mammary Ducts with Micro-Endoscope called Mammary Ductoscopy. Indication:- Nipple Discharge. In this case Papilloma seen quite clearly. Biopsy can also be possible with Ductoscopy. Mammary Ductoscopy is very useful for diagnosis of Breast Cancer in early stage.
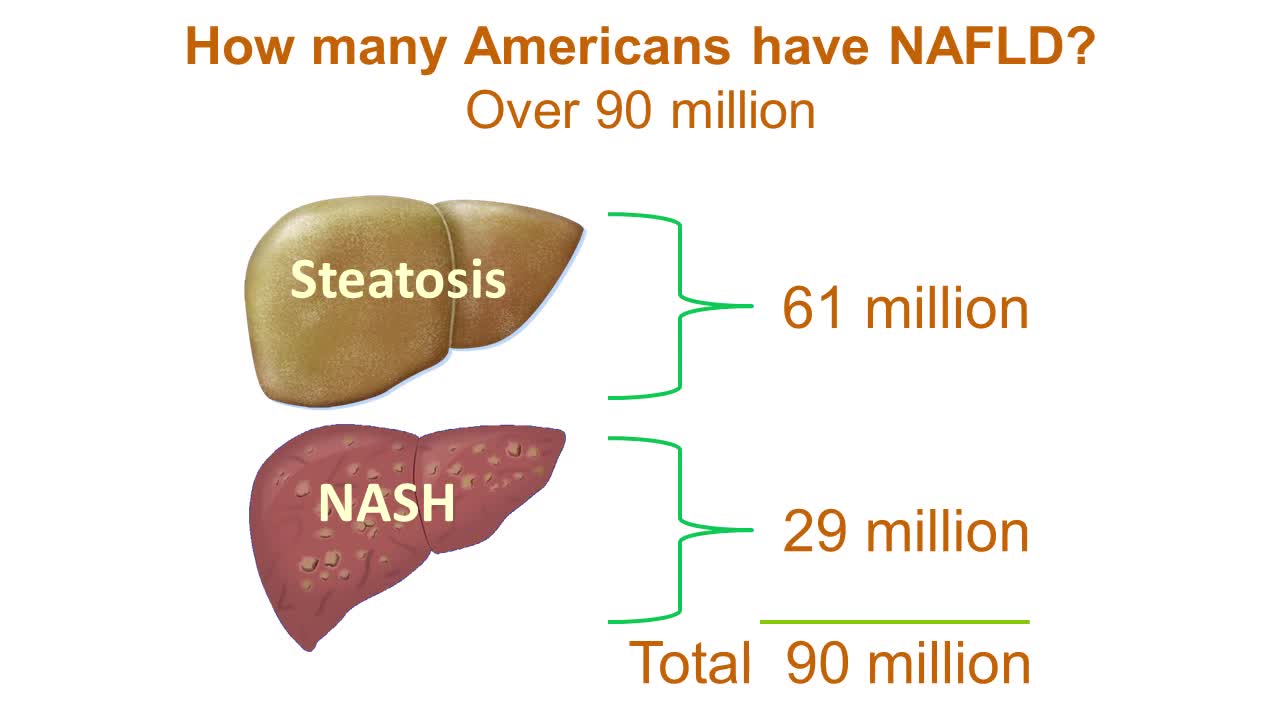
Nonalcoholic fatty liver disease is an umbrella term for a range of liver conditions affecting people who drink little to no alcohol. As the name implies, the main characteristic of nonalcoholic fatty liver disease is too much fat stored in liver cells. Nonalcoholic steatohepatitis, a potentially serious form of the disease, is marked by liver inflammation, which may progress to scarring and irreversible damage. This damage is similar to the damage caused by heavy alcohol use. At its most severe, nonalcoholic steatohepatitis can progress to cirrhosis and liver failure Nonalcoholic fatty liver disease is increasingly common around the world, especially in Western nations. In the United States, it is the most common form of chronic liver disease, affecting an estimated 80 to 100 million people. Nonalcoholic fatty liver disease occurs in every age group but especially in people in their 40s and 50s who are at high risk of heart disease because of such risk factors as obesity and type 2 diabetes. The condition is also closely linked to metabolic syndrome, which is a cluster of abnormalities including increased abdominal fat, poor ability to use the hormone insulin, high blood pressure and high blood levels of triglycerides, a type of fat. Nonalcoholic fatty liver disease care at Mayo Clinic Request an Appointment at Mayo Clinic Symptoms & causes Aug. 23, 2016 Print Share on: Facebook Twitter References Related Magnetic resonance elastography Nonalcoholic fatty liver disease Overview Symptoms & causes Diagnosis & treatment Diagnosis Treatment Departments & specialties Expertise & rankings Locations, travel & lodging Clinical trials Research Costs & insurance Preparing for your appointment Self-management More about In-Depth Multimedia Resources News from Mayo Clinic Advertisement

Brushing flossing and rinsing -the winning combination for preventing gingivitis

Watch that video of Dissection Inside Fat Body

Follow along on a typical day with UCSF Medical Center's chief of cardiothoracic surgery Dr. Tom Nguyen. Take a walk on rounds with his team as they check on patients who are recovering or preparing for heart valve surgeries to treat conditions such as mitral valve prolapse and mitral regurgitation. Get a glimpse into the operating room as Dr. Nguyen and his team use the latest non-invasive techniques to help patients achieve the best outcomes.
0:00 Surgeon begins day with morning report
0:53 Meet with fellows and visit patients
1:28 Surgeon thoughts on his practice
Minimally Invasive Surgeries
2:09 Mitral valve replacement for mitral stenosis
3:11 Mitral valve repair for AFib and mitral regurgitation
3:36 Stopping the heart
4:15 Culture 1 - Everyone's voice matters
4:45 Mitral valve repair for heart murmur
5:12 Culture 2 - Patient first
To view more UCSF videos relating to Mitral Regurgitation Treatment and Aortic Stenosis Treatment view:
Mitral Regurgitation Treatment Options https://youtu.be/7nUUOMx4tJ0
Aortic Stenosis Treatment Options https://youtu.be/A2rZK0oFWcc
If you want to learn more about the Cardiac Surgery clinic and to request an appointment visit: https://www.ucsfhealth.org/cli....nics/cardiac-surgery
#dayinthelife #heartsurgeon #heartsurgery #CardiacSurgery #Cardiology #ucsf #drnguyen#ucsfhealth #Cardiothoracic
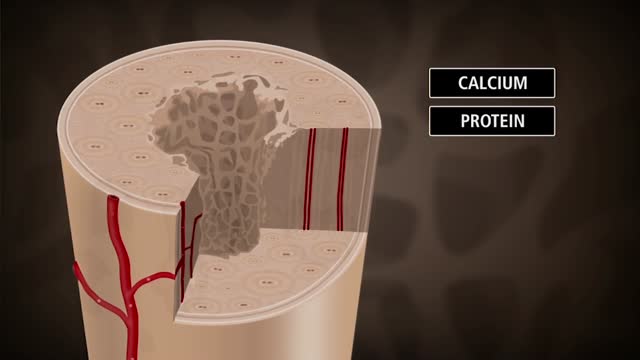
Bone is not a static part of the body — it's constantly being resorbed (broken down) and formed throughout your life. Your entire skeleton is replaced about every decade, according to the NIH. During your childhood and teenage years, bone formation occurs more quickly than bone resorption, resulting in growth. You reach your maximum bone density and strength around age 30, after which bone resorption slowly overtakes bone formation. Osteoporosis develops when there's an abnormal imbalance between bone resorption and formation — that is, resorption occurs too quickly, or formation too slowly.
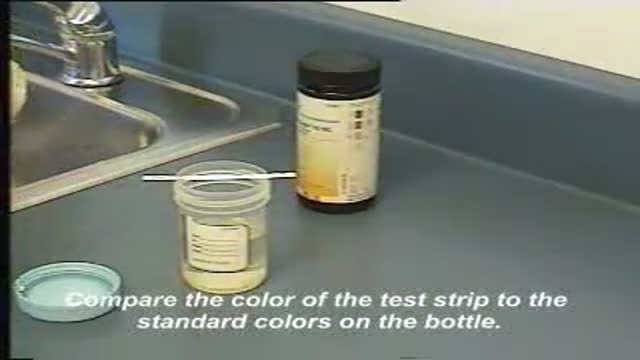
This video demonstrates how use a commercially-prepared "dip-stick" to test a random urine specimen for the presence of protein or glucose.

Watch that Complete Chopped Hand Re-Implantation Surgery
A natural, unmedicated approach to labor and birth will suit you best if you want to remain in control of your body as much as possible, be an active participant throughout labor, and have minimal routine interventions such as continuous electronic monitoring. If you choose to go this route, you accept the potential for pain and discomfort as part of giving birth. But with the right preparation and support, women often feel empowered and deeply satisfied by natural childbirth.

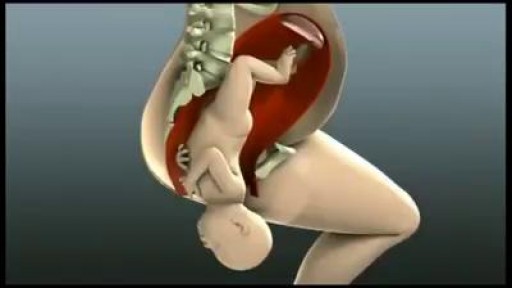
Most babies will move into delivery position a few weeks prior to birth, with the head moving closer to the birth canal. When this fails to happen, the baby’s buttocks and/or feet will be positioned to be delivered first. This is referred to as “breech presentation.” Breech births occur in approximately 1 out of 25 full-term births.
