- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
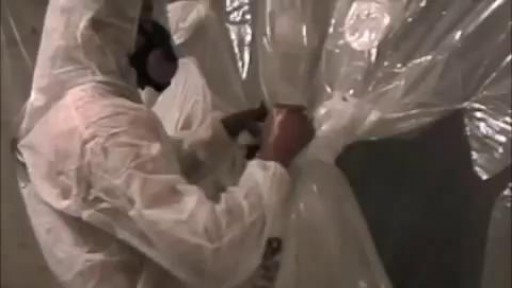
Every owner of a building where asbestos abatement activity occurs is responsible for the performance of the asbestos abatement activities by his/her agent, contractor, employee, or other representative. Each building owner is responsible for determining the amount of asbestos-containing material that may be disturbed during the course of work. The size and scope of the overall project, with particular reference to the total amount of asbestos-containing material that will be disturbed determines the reporting or filing requirements established in the Asbestos Control Program Rules. An asbestos project is defined as any form of work that will disturb more than 25 linear feet or more than 10 square feet of asbestos-containing material.

Meckel's Diverticulum is a vestigeal remnant of vitellointestinal duct. Its a true diverticulum as it contains all three layers of intestine. It is usually presents at anti mesenteric burder. Usually 2 cm (range 1- 12 cm ) in length, found in 2 % of population , and situated around 2 feet of Ileaocecal junction. 50 % cases it contains gastric mucosa , but may also contain colonic, duodenal or pancreatic mucosa .male : female ration in symptomatic cases is 3 : 1.It may mimic acute appendicitis, so in cases where one is going for surgery for appendicitis , must search for meckel's diverticulum........

A pacemaker insertion is the implantation of a small electronic device that is usually placed in the chest (just below the collarbone) to help regulate slow electrical problems with the heart.

Huge Pimple Draining

Skin Whitening Tips, Vitamin C For Skin Whitening, Skin Whitening Before And After, Skin Whitening. http://skin-whitening.good-info.co Each and every person wants a clean and radiant skin. Some spend fortunes on cosmetic products that will lighten the skin and remove all the imperfections, others spend their money on esthetic operations in the hope that their skin will look perfect. Lastly, there are people trying to fake a healthy skin by using all kinds of makeup that will cover the imperfections and leave the impression that the skin is healthy and has no scars, wrinkles or spots. All these people are looking for a way through which they can make their skin look good. Yet, what they have not taken into consideration is the power of natural ingredients. Fruits, vegetables and products coming from animals are great sources of anti-oxidants and are rich in substances which can whiten the skin, moisturize it, attenuate the fine lines and wrinkles and give it elasticity. There are many natural ingredients which can be used in order to remove the dark spots and whiten the skin and as many reasons to start trying them. The first reason for which you should try the natural skin whitening ingredients is the fact that they have no side effects. Because most of the ingredients with which the homemade skin whitening recipes are made are natural, and are used in our everyday diet, the human body tolerates them very well and responds positively to the ingredients they contain. In addition to that, because you know what you put in that homemade recipe, you know if your skin will going to react negatively to it. There are certain products (fruits, vegetables, animal products) to which certain people are allergic. Exclude those ingredients from your recipes and you know you will obtain a 100% safe homemade product. Click Here. http://skin-whitening.good-info.co
http://sweating-cure.info-pro.co/ --- Why Do I Sweat So Much, How To Stop Sweaty Armpits, How To Stop Your Hands From Sweating. The 4 Step Formula to Stop Sweating How to Stop Excessive Sweating in Minutes There is a simple 4 step formula you need to implement immediately if you want to finally end your excessive sweating and put a stop to the constant embarrassment. These 4 steps are absolutely essential if you’re having trouble controlling the endless perspiration. Don’t prolong the problem any longer. Take action with these simple steps right now. http://sweating-cure.info-pro.co/

How To Help Your Child Learn To Read, Help My Child Learn To Read, Best Way To Teach Reading---- http://children-learning-reading.good-info.co -- how to help your child learn to read - Help My Child Learn to Read The ability to read is vital for success. It helps your child succeed in school, helps them build self-confidence, and helps to motivate your child. Being able to read will help your child learn more about the world, understand directions on signs and posters, allow them to find reading as an entertainment, and help them gather information. Learning to read is very different from learning to speak, and it does not happen all at once. There is a steady progression in the development of reading ability over time. The best time for children to start learning to read is at a very young age - even before they enter pre-school. Once a child is able to speak, they can begin developing basic reading skills. Very young children have a natural curiosity to learn about everything, and they are naturally intrigued by the printed texts they see, and are eager to learn about the sounds made by those letters. You will likely notice that your young child likes to look at books and thoroughly enjoys being read to. They will even pretend to behave like a reader by holding books and pretend to read them. As parents, you're the most important first step in your children's journey into the wonderful world of reading. It is up to you to create the most supportive environment that turns your child on to reading - such as reading aloud to them often during the day and before bedtime, and placing age appropriate books for children around the house, so that the child will have access to plenty of books. Reading often to your child will help develop their interest in books and stories, and soon they will want to read stories on their own. >>Teach your child to read and enable your child to become a fast and fluent reader! Click here to help your child learn to read http://children-learning-reading.good-info.co

Watch that video of Ingrown hair turns into Horrible 140-pound tumor in man’s stomach

Endoscope-assisted pocket grafting of autologous collagen for correction of facial wrinkles

Liposuction for weight loss with Abdominoplasty and Body Lifting
Weight Reduction Surgery Animation 3D

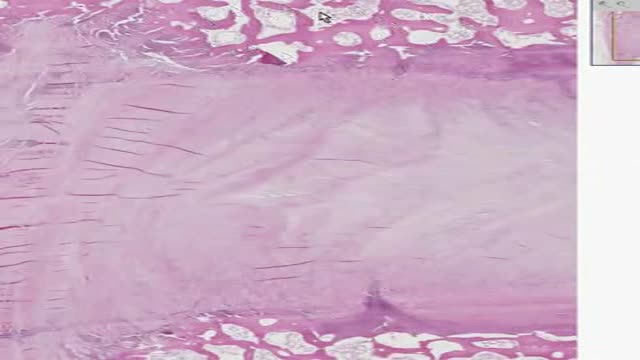
Histology of Intervertebral Disk
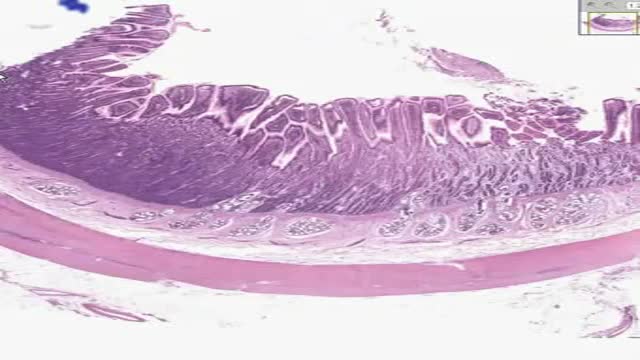
Histology of Small Intestine Duodenum
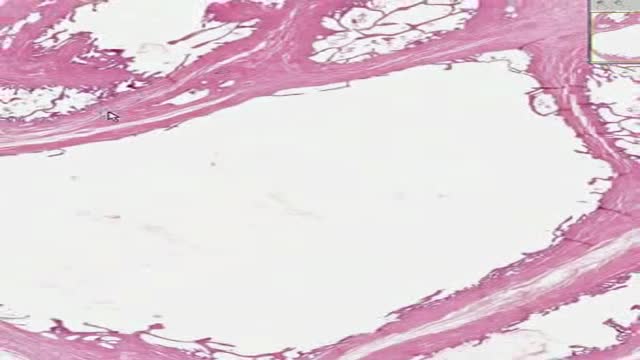
Histology of Seminal Vescicles

See the War Inside Your Body

How to Tell if Knee Pain is Meniscus or Ligament Injury
Youtube Channel: https://www.youtube.com/user/physicaltherapyvideo
Website: https://bobandbrad.com/
Bob and Brad discuss how to tell if you are having a meniscus or ligament injury. They also include some tests you can try at home to distinguish the two.
Interested in learning about the products mentioned in today's video:
1) Booyah Stik: https://store.bobandbrad.com
This Week's Giveaway:
Giveaway Link: https://bobandbrad.com/bob-and-brad-giveaways
Purchase Link: https://store.bobandbrad.com/
Discount: 15% off your entire purchase using code BOBBRADFAN
This giveaway is open to all of our fans worldwide!!
If you order a grip & forearm strengthener now AND you end up winning the giveaway, we will reimburse your purchase! No need to hold off on purchasing Bob and Brad’s Grip & Forearm Strengthener!
Our videos offer the best "get fit , stay healthy, and pain-free" information directed toward people 0 to 101 years old. Physical Therapists Bob Schrupp and Brad Heineck have over 50 years of combined com/shop/physicaltherapyvideo We try to add a twist of our humor into each video in our quest to be the "Most Famous experience in the physical therapy field. Not only will these videos provide outstanding health information on treating yourself at home, we also do product reviews. For our favorite products on Amazon click on this link. https://www.amazon. Physical Therapists on the Internet" In our opinion of course!!! Subscribe to us now and join the fun.
Visit us on our other social media platforms:
Website: https://bobandbrad.com/
Facebook: https://www.facebook.com/BobandBrad/
Instagram: https://www.instagram.com/officialbobandbrad/
Twitter: https://twitter.com/ptfamous
Bob and Brad’s Products:
Grip and Forearm Strengthener: https://store.bobandbrad.com/
Wall Anchor: https://store.bobandbrad.com/
Booyah Stik: https://store.bobandbrad.com
Knee Glide: https://amzn.to/2WnSPU1
Check out our shirts, mugs, bags and more in our Bob and Brad merchandise shop here:
https://shop.spreadshirt.com/bob-brad
Check out other products Bob and Brad Love:
https://www.amazon.com/shop/physicaltherapyvideo?listId=3581Z1XUVFAFY
Check out The Bob & Brad Crew on YouTube by clicking here:
https://www.youtube.com/c/thebobbradcrew
Want to help translate our videos? We would so love the help!
http://www.youtube.com/timedtext_cs_panel?c=UCmTe0LsfEbpkDpgrxKAWbRA&tab=2
Medical Disclaimer
All information, content, and material of this website is for informational purposes only and are not intended to serve as a substitute for the consultation, diagnosis, and/or medical treatment of a qualified physician or healthcare provider.
Affiliate disclaimer:
Keep in mind that we may receive commissions when you click our links and make purchases. However, this does not impact our reviews and comparisons. We are highly selective in our products and try our best to keep things fair and balanced in order to help you make the best choice for you.

Father & Mom feel their baby the same

Birthmark Removal with Laser
