- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
There are several reasons that your doctor may recommend that you have your spleen removed. These include having: a spleen that’s damaged from injury an enlarged spleen or ruptured spleen, which can occur from trauma certain rare blood disorders cancer or large cysts of the spleen infection
Symptoms of blood clots in specific body locations are as follows: Symptoms of blood clots in legs (deep vein thrombosis (DVT) are pain, redness, and swelling. Symptoms of an arterial blood clot in a limb (leg or arm) include pain, pale color, and coolness to the touch. and the leg is cool and pale.
Surgeon performs a dissection of the transverse process during spine surgery, explaining the benefits of including the AQUAMANTYS System from Salient Surgical Technologies during the procedure. The AQUAMANTYS System uses Salient's patented TRANSCOLLATION technology, which has been clinically shown to reduce blood loss and lower blood transfusion rates when used during surgery.

An animated description of the composition of bones.
Visit www.orthofilms.com for more videos and info.
An animation showing vaginal childbirth (delivery)
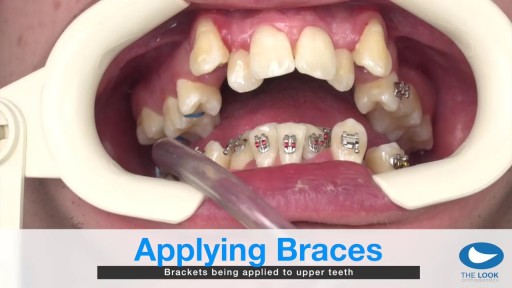
How teeth braces are put

Examination of the abdomen from the USMLE collection
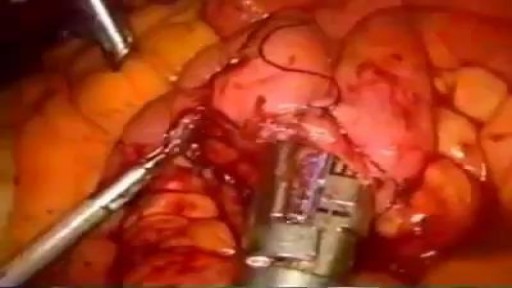
Gunshot Wound to the Abdomen: Laparoscopic Exploration and Repair of Small Bowel Injury.

World-renowned surgeons at Shriners Hospitals for Children – Northern California provide complex pediatric surgery for children one-year and older with congenital and acquired conditions. Children from throughout the Western United States with chest wall malformations, gastro-intestinal disease, ano-rectal disorders, urologic conditions and other complex surgical needs benefit from the expert care. The pediatric surgery team is devoted to the development of innovative and minimally invasive surgical techniques.
Though the risk of HIV transmission through oral sex is very low, but several factors might increase the risk, including sores in the mouth or vagina or on the penis, bleeding gums, having an oral contact with menstrual blood, and the presence of other sexually transmitted diseases. But still the risk is low. by the way better to think twice before having the Oralsex with strangers. because you are not safe 100%.

Debridement is the removal of necrotic tissue, foreign debris, bacterial growth, callus, wound edge, and wound bed tissue from chronic wounds in order to stimulate the wound healing process. Stimulation of wound healing mediated by debridement is thought to occur by the conversion of a chronic non-healing wound environment to an acute healing environment through the removal of cells that are not responsive to endogenous healing stimuli. Debridement is used commonly in standard wound treatment of diabetic foot ulcers (DFUs). Methods of debridement include surgery (sharp debridement), chemical debridement (antiseptics, polysaccharide beads, pastes), autolytic (hydrogels, hydrocolloids and transparent films), biosurgery (maggots), mechanical (hydrodebridement), and biochemical debridement (enzyme preparations). Callus is a buildup of keratinized skin formed under conditions of repeated pressure or friction and may contribute to ulcer formation by creating focal areas of high plantar pressure. The debridement of callus has been proposed to be relevant for both treatment and prevention of DFU. The purpose of this report is to retrieve and review existing evidence of comparative clinical effectiveness of different methods of debridement for the treatment of DFUs. Additionally examined in this report is the clinical effectiveness for treatment and prevention of DFU using callus debridement. Cost-effectiveness, and existing debridement guidelines for the treatment of DFUs will also be reviewed.

Internal hemorrhoids and loose rectal mucosa may block the exposure during the purse string suturing in stapled hemorrhooidopexy, and this may cause some complications. To retract the prolapsing rectal mucosa we modified the purse string anoscope of the PPH01 kit (Ethicon-Endosurgery, Cincinnati, O...H, USA) and produced a special anoscope. The open part of the purse string suture anoscope is covered by transparent acrylic (Orthoacryl�, Dentaurum, Pforzheim, Germany). The covering material had complete cylindrical outer and inner surfaces and was thin enough to let the anoscope easily rotate in the anal dilator and to let the 26 mm curved, round bodied needle of the 2/0 polypropilene suture move in the anoscope. A window, 3 cm long and 3-4 mm wide, was opened at the angled part of the anoscope 2 cm to the tip of the anoscope. This special anoscope was used for the purse string suture during stapled hemorrhoidopexy procedure in five patients. No postoperative complications, early or late, were encountered, and we propose that stapled hemorrhoidopexy procedure can be applied more easily by using this special anoscope.

What is hemodialysis, and why would someone need it? How does hemodialysis work? Can people perform hemodialysis at home? John Kevin Tucker, M.D., Nephrologist at Brigham and Women's Hospital and Vice President for Education at Mass General Brigham, discusses hemodialysis and how it helps people who have lost their kidney function to maintain normal lives.
Subscribe Link: https://www.youtube.com/channe....l/UCYrLjATd88gPwIKnt
0:00 - Intro
0:26 - The Condition
2:06 - Hemodialysis: How It Works
4:37 - In-Center Hemodialysis Care Team
About Mass General Brigham:
Mass General Brigham combines the strength of two world-class academic medical centers, five nationally ranked specialty hospitals, 11 community hospitals, and dozens of health centers. Our doctors and researchers accelerate medical breakthroughs and drive innovations in patient care. They are leaders in medical education, serving as Harvard Medical School faculty and training the next generation of physicians. Mass General Brigham’s mission is to deliver the best, affordable health care to patients everywhere. Together, we transform the health of our communities and beyond.
#MassGeneralBrigham #MGB #Hemodialysis
Visit Mass General Brigham: https://www.massgeneralbrigham.org/
Find us on social:
Twitter: https://twitter.com/MassGenBrigham
Instagram: https://www.instagram.com/massgeneralbrigham/
Facebook: https://www.facebook.com/MassGeneralBrigham/
LinkedIn: https://www.linkedin.com/compa....ny/mass-general-brig
Mass General Brigham:
https://www.youtube.com/massgeneralbrigham
Kidney Failure: Signs, Dialysis Options, and Hemodialysis Explained | Mass General Brigham
https://youtu.be/azy7yc19QYQ

This innovative minimally invasive technique can remove large tumors located deep in the brain
To learn more, please visit http://brainsurgery.upmc.com
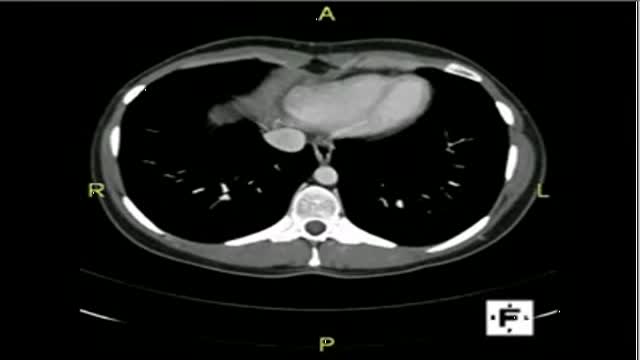
The video will describe anatomical structures as seen on a CT scan. Please see discalimer on my website.

As a doctor many people ask me about masturbation and if it is harmful or not. As a doctor you have already been asked this and this video will give you some hints

Breast cancer is a malignant tumor that develops from the cells of
the breast. It is the most common type of cancer among women in
the United States. It is most often curable when found early. The
normal breast consists of three main components: the lobules
(milk-producing glands), the ducts (thin tubes that connect the
lobules to the nipple) and the stroma (fatty tissue and ligaments
surrounding the ducts and lobules, blood vessels, and lymphatic
vessels). About 80% of breast cancers start in the ducts.
Watch that video to know the Abnormal Female Genital Bleeding Causes

Hypertensive emergencies encompass a spectrum of clinical presentations in which uncontrolled blood pressures lead to progressive or impending end-organ dysfunction. In these conditions, the BP should be lowered aggressively over minutes to hours. Neurologic end-organ damage due to uncontrolled BP may include hypertensive encephalopathy, cerebral vascular accident/cerebral infarction, subarachnoid hemorrhage, and/or intracranial hemorrhage.[1] Cardiovascular end-organ damage may include myocardial ischemia/infarction, acute left ventricular dysfunction, acute pulmonary edema, and/or aortic dissection. Other organ systems may also be affected by uncontrolled hypertension, which may lead to acute renal failure/insufficiency, retinopathy, eclampsia, or microangiopathic hemolytic anemia.[1] With the advent of antihypertensives, the incidence of hypertensive emergencies has declined from 7% to approximately 1% of patients with hypertension.[2] In addition, the 1-year survival rate associated with this condition has increased from only 20% (prior to 1950) to a survival rate of more than 90% with appropriate medical treatment
