Top Videos
“Complete cure from groin hernia is now possible with Dr.Desarda's repair technique.......” Mesh is a foreign body. Therefore, its use in hernia repairs is known to cause all sorts of complications like pain, recurrence, infection etc. We have developed an innovative new technique of inguinal hernia repair without mesh. It uses your own body muscle for repair and gives virtually complete cure from inguinal hernia problem. An undetached strip of the external oblique aponeurosis is stitched on the weak area between the muscle arch and the inguinal ligament to form a new, strong and physiologically dynamic posterior wall that gives protection and prevents re-herniation. Normally patient goes home in a day after surgery and can drive car and go to office in 3-4 days time. This "Dr.Desarda's hernia repair" is now followed in many countries all over the world. We are surprised to see the enquiries from many patients in the developed countries asking for this repair in their country. This is because this operation does not use any foreign body like mesh for repair and therefore there are no complications that are seen in mesh repairs. A visit to Topix or other hernia forums show thousands of posts showing sufferings of many patients due to mesh repairs. But still why surgeons from developed countries are interested in mesh repairs is a big question for us. Please visit our website for more details: http://herniasurgery.tripod.com Our cell number: +91 9373322178
A video showing clinical examination of the thyroid gland

Varicose veins are caused by weakened valves and veins in your legs. Normally, one-way valves in your veins keep blood flowing from your legs up toward your heart. When these valves do not work as they should, blood collects in your legs, and pressure builds up. The veins become weak, large, and twisted.

A new and safer method of inserting a Foley catheter suprapubically. The technique allows the insertion to be carried out in an Outpatient setting, thus saving time, cost and effort. By using the Seldinger technique, the product reduces the chances of bowel or bladder perforation and resultant morbidity.
The product has been chosen by The NHS National Technology Adoption Centre to help facilitate adoption of the product.
See www.mediplus.co.uk for more information
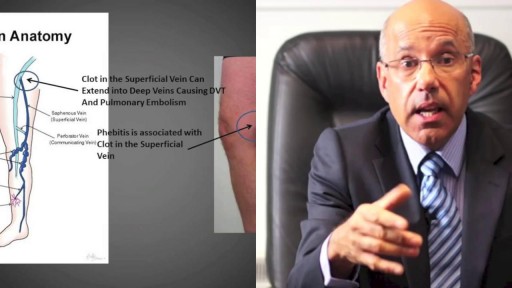
Phlebitis may occur with or without a blood clot. It can affect surface or deep veins. When caused by a blood clot, it's called thrombophlebitis. Trauma to the vein, for instance from an IV catheter, is a possible cause. Symptoms include redness, warmth, and pain in the affected area. Treatments may include a warm compress, anti-inflammatory medication, compression stockings, and blood thinners.

Dr. Ankur Gupta of the Virginia Eye Institute discusses LASIK eye surgery as a method of correcting refractive errors. LASIK was first performed in Virginia on an FDA-approved laser by a VEI surgeon in 1996. Today, Virginia Eye Institute offers both conventional LASIK and custom LASIK with the bladeless IntraLase laser to precisely sculpt your cornea to correct refractive errors.
For more information on the services and procedures offered at Virginia Eye Institute please visit: https://goo.gl/6nX4RZ
THE CONTENT IN THIS VIDEO IS GENERAL IN NATURE AND DOES NOT SUBSTITUTE PROFESSIONAL MEDICAL ADVICE. The content on our website including, but not limited to, text, images, and videos is for informational and educational purposes only. Although we work hard to provide accurate general information, it is not a substitute for professional medical advice or consultations with healthcare professionals, and does not establish any kind of provider-patient relationship. Our website information is not intended to make any promises about the results of our products and services. We are not liable for actions taken based on content found on our website. If you are seeking medical advice, diagnoses, or treatment, we encourage you to call 804-287-2020 to make an appointment with one of our providers for your individualized care plan.

This video clip shows nasolabial cyst being excised under local anesthesia

How to Use a Menstrual Cup Fold and hold. Always start by washing your hands. ... Insert and ensure. As with tampons, gently insert the folded cup into your vagina, tilting it back to the base of your spine. ... Use it up to twelve hours. ... Remove and empty. ... Re-insert.

An amputation is the removal of an extremity or appendage from the body. Amputations in the upper extremity can occur as a result of trauma, or they can be performed in the treatment of congenital or acquired conditions. Although successful replantation represents a technical triumph to the surgeon, the patient's best interests should direct the treatment of amputations. The goals involved in the treatment of amputations of the upper extremity include the following : Preservation of functional length Durable coverage Preservation of useful sensibility Prevention of symptomatic neuromas Prevention of adjacent joint contractures Early return to work Early prosthetic fitting These goals apply differently to different levels of amputation. Treatment of amputations can be challenging and rewarding. It is imperative that the surgeon treat the patient with the ultimate goal of optimizing function and rehabilitation and not become absorbed in the enthusiasm of the technical challenge of the replantation, which could result in poorer outcome and greater financial cost due to lost wages, hospitalization, and therapy.

Cystoscopy

Mobile scanner detects disease from a drop of blood by nanotechnology

Squamous cell carcinomas typically appear as persistent, thick, rough, scaly patches that can bleed if bumped, scratched or scraped. They often look like warts and sometimes appear as open sores with a raised border and a crusted surface. In addition to the signs of SCC shown here, any change in a preexisting skin growth, such as an open sore that fails to heal, or the development of a new growth, should prompt an immediate visit to a physician.

This 35 years old man lost his right wrist in metal lathe cut machine. the video is taken about 2 years after replantation. You can see another videos in my site: https://drliaghatclinic.com, https://instagram.com/liaghatclinic, https://t.me/liaghatclinic
A peak flow meter is an inexpensive, portable, handheld device for those with asthma that is used to measure how well air moves out of your lungs. Measuring your peak flow using this meter is an important part of managing your asthma symptoms and preventing an asthma attack.
Closed Reduction of Distal Radius Fractures - Discussion: (distal radius fracture menu) - closed reduction & immobilization in plaster cast remains accepted method of treatment for majority of stable distal radius frx; - unstable fractures will often lose reduction in the cast and will slip back to the pre-reduction position; - patients should be examined for carpal tunnel symptoms before and after reduction; - carpal tunnel symptoms that do not resolve following reduction will require carpal tunnel release; - cautions: - The efficacy of closed reduction in displaced distal radius fractures. - Technique: - anesthesia: (see: anesthesia menu) - hematoma block w/ lidocaine; - w/ hematoma block surgeon should look for "flash back" of blood from hematoma, prior to injection; - references: - Regional anesthesia preferable for Colles' fracture. Controlled comparison with local anesthesia. - Neurological complications of dynamic reduction of Colles' fractures without anesthesia compared with traditional manipulation after local infiltration anesthesia. - methods of reduction: - Jones method: involves increasing deformity, applying traction, and immobilizing hand & wrist in reduced position; - placing hand & wrist in too much flexion (Cotton-Loder position) leads to median nerve compression & stiff fingers; - Bohler advocated longitudinal traction followed by extension and realignment; - consider hyper-extending the distal fragment, and then translating it distally (while in extended position) until it can be "hooked over" proximal fragment; - subsequently, the distal fragment can be flexed (or hinged) over the proximal shaft fragment; - closed reduction of distal radius fractures is facilitated by having an assistant provide counter traction (above the elbow) while the surgeon controls the distal fragment w/ both hands (both thumbs over the dorsal surface of the distal fragment); - flouroscopy: - it allows a quick, gentle, and complete reduction; - prepare are by prewrapping the arm w/ sheet cotton and have the plaster or fibroglass ready; - if flouroscopy is not available, then do not pre-wrap the extremity w/ cotton; - it will be necessary to palpate the landmarks (outer shaped of radius, radial styloid, and Lister's tubercle, in order to judge success of reduction; - casting: - generally, the surgeon will use a pre-measured double sugar sugar tong splint, which is 6-8 layers in thickness; - more than 8 layers of plaster can cause full thickness burns: - reference: Setting temperatures of synthetic casts. - position of immobilization - follow up: - radiographs: - repeat radiographs are required weekly for 2-3 weeks to ensure that there is maintenance of the reduction; - a fracture reduction that slips should be considered to be unstable and probably require fixation with (pins, or ex fix ect.) - there is some evidence that remanipulation following fracture displacement in cast is not effective for these fractures; - ultimately, whether or not a patient is satisfied with the results of non operative treatment depends heavily on th


Clogged leg arteries can be opened through a minimally invasive procedure with the SILVERHAWK, a mini drill with a tiny rotating blade for cutting away plaque. The procedure only involves a tiny puncture in the patient's groin. ~ Detroit Medical Center


An untreated hepatic abscess is nearly uniformly fatal as a result of complications that include sepsis, empyema, or peritonitis from rupture into the pleural or peritoneal spaces, and retroperitoneal extension. Treatment should include drainage, either percutaneous or surgical. Antibiotic therapy as a sole treatment modality is not routinely advocated, though it has been successful in a few reported cases. It may be the only alternative in patients too ill to undergo invasive procedures or in those with multiple abscesses not amenable to percutaneous or surgical drainage. In these instances, patients are likely to require many months of antimicrobial therapy with serial imaging and close monitoring for associated complications.

Vesicoureteral (ves-ih-koe-yoo-REE-tur-ul) reflux is the abnormal flow of urine from your bladder back up the tubes (ureters) that connect your kidneys to your bladder. Normally, urine flows only down from your kidneys to your bladder. Vesicoureteral reflux is usually diagnosed in infants and children. The disorder increases the risk of urinary tract infections, which, if left untreated, can lead to kidney damage. Vesicoureteral reflux can be primary or secondary. Children with primary vesicoureteral reflux are born with a defect in the valve that normally prevents urine from flowing backward from the bladder into the ureters. Secondary vesicoureteral reflux is due to a urinary tract malfunction, often caused by infection. Children may outgrow primary vesicoureteral reflux. Treatment, which includes medication or surgery, aims at preventing kidney damage.
