- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
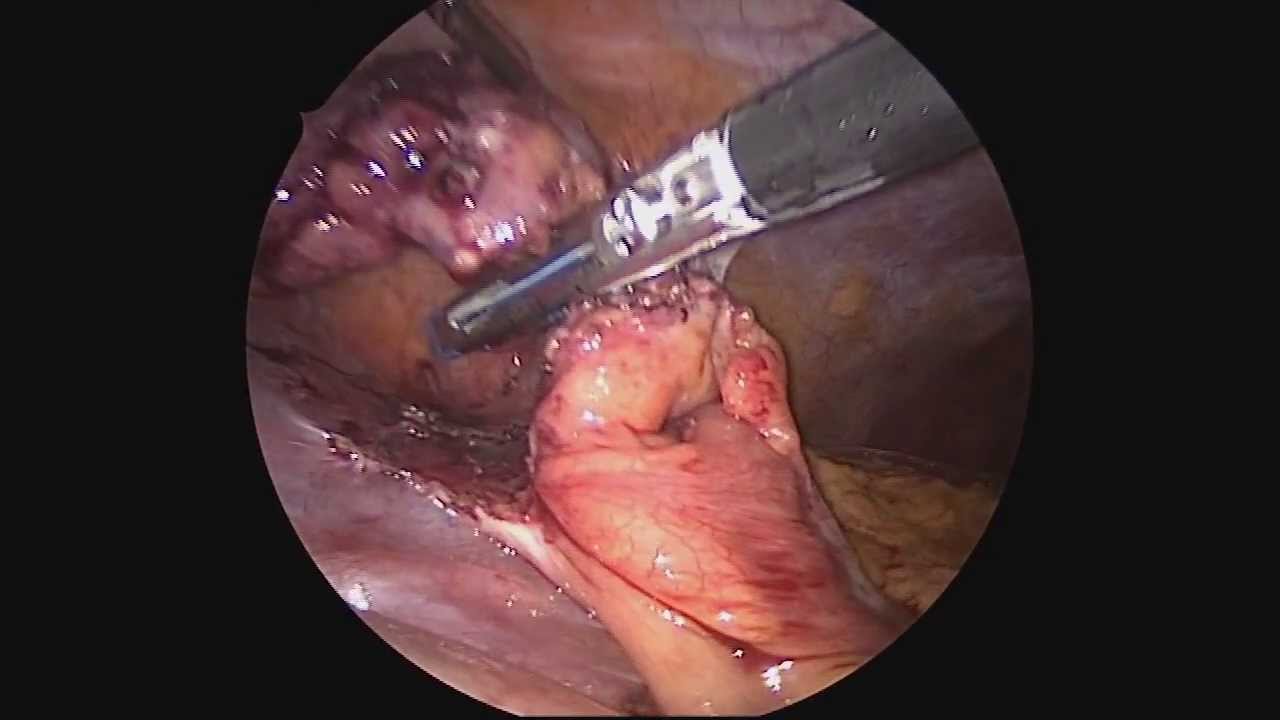
Dr. Celia Divino, Chief, Division of General Surgery at The Mount Sinai Hospital, performs a laparoscopic appendectomy. Visit the Division of General Surgery at http://bit.ly/18z944M. Click here to learn more about Dr. Celia Divino http://bit.ly/12RF0ee

OB_A_1013
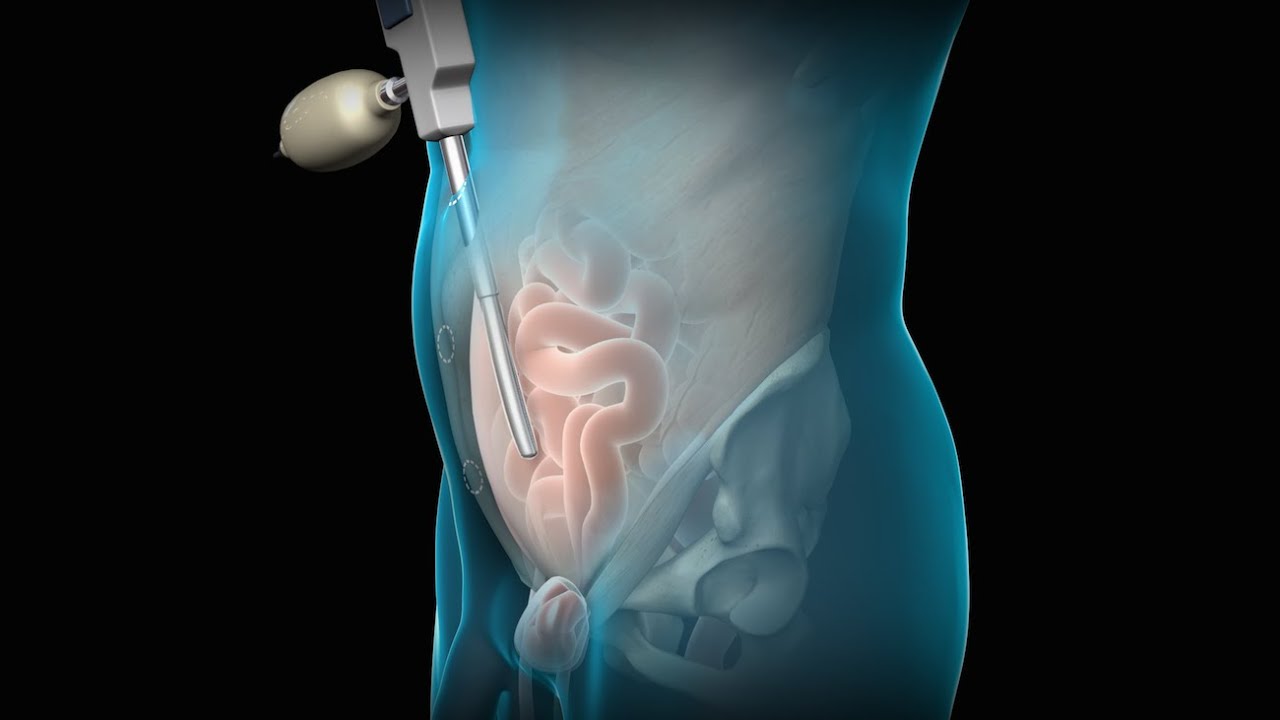
3D animation depicting the operating room and initial procedure preparing the patient for a laparoscopic hysterectomy. The patient is prepped and draped in the usual fashion and surrounded by the surgeon and surgical assistants. The skin is elevated, an infraumbilical incision is made, a trocar port is inserted through the incision and the abdomen is insufflated. Finally, a laparoscope is inserted into the port to allow for direct visualization of the uterus and the surgery can begin.
To view more animations and exhibits, visit our medical library: https://www.trialexhibitsinc.c....om/library/multimedi
Contact us on your next case for consulting, trial graphics, animations, medical illustrations or presentation services. 800-591-1123 [a]www.trialex.com[/a]
This video is for reference only. The video may not be otherwise used, reproduced nor modified. For more information to purchase a copy or permission to use this animation on your next case, project, website or TV, contact us at [a]www.trialex.com[/a] or 800-591-1123.
Copyright @ Trial Exhibits, Inc.

UChicago Medicine organ transplant surgeon Dr. Rolf Barth explains a how the laparoscopic donor nephrectomy – also known as the single-port nephrectomy – procedure works to remove an organ donor’s kidney from their body to be transplanted into a recipient. This minimally invasive kidney donor transplant surgery allows living organ donors the get back to their lives more quickly than the traditional approach and leaves them with a nearly invisible scar in the belly button.
Learn more about living kidney donation: https://www.uchicagomedicine.o....rg/conditions-servic
To license this video for patient education or content marketing, visit: http://www.nucleushealth.com/?utm_source=youtube&utm_medium=video-description&utm_campaign=tephernia-030615
An inguinal hernia is a bulging of the intestine through a defect or weak spot in the wall of the lower abdomen. This video shows how inguinal hernias form and how they are treated.
#TotalExtraperitonealLaparoscopicInguinalHerniaRepair #TEP #laparoscopy
ANCE00200

Visit our website to learn more about using Nucleus content for patient engagement and content marketing: http://www.nucleushealth.com/
#LaparoscopicColectomy #ColonSurgery #LargeIntestine
A colectomy is usually done to treat diseases that inflame your colon, a bowel obstruction, colon cancer, or a damaged or injured colon. The anatomy of the colon, and the laparoscopic procedure done to remove a portion of the colon, are depicted.
ANH18221

Laparoscopic surgery is minimally-invasive (keyhole) surgery and it is performed through very small incisions, using a camera to guide the surgeon during the procedure. Miss Sarah Mills, a top colorectal surgeon, explains why laparoscopic surgery is performed over alternative methods.
Make an appointment with Miss Sarah Mills here: https://www.topdoctors.co.uk/doctor/sarah-mills

Vatche, Minassian, MD, MPH, Chief of Urogynecology, and Sarah Cohen, MD, MPH, Director of the Minimally Invasive Gynecologic Surgery Fellowship Program at Brigham and Women’s Hospital, perform a laparoscopic burch colposuspension, a procedure used to correct stress urinary incontinence.
Stress urinary incontinence is one of the most common types of incontinence and is characterized by urinary leakage during physical activities including coughing, sneezing, exercising, lifting, and laughing. As the condition progresses, it can become severe enough to happen with simple acts such as bending and walking. This condition is due to an anatomic weakness of the bladder neck which typically maintains the seal of urine during activity. Stress incontinence can result from a variety of conditions including vaginal childbirth, aging, menopause and obesity. As this is an anatomic condition, primary treatment may involve pelvic floor exercises and/or minimally invasive surgery.
Learn more about treatment for stress urinary incontinence:
Division of Urogynecology: http://www.brighamandwomens.or....g/Departments_and_Se
Division of Minimally Invasive Gynecologic Surgery: http://www.brighamandwomens.or....g/Departments_and_Se

For more videos, please visit:
http://surgicalfilmatlas.mssm.edu/


Dr. Erica Hodgman discusses pediatric surgery at the Johns Hopkins Children's Center Pediatric General Surgery program, what common surgeries the program specializes in, what makes the program unique and her work as a pediatric surgeon. #PediatricSurgery #JohnsHopkinsChildrenCenter
Questions Answered:
0:03 Describe the pediatric general surgery division at Johns Hopkins Children's Center.
1:00 What makes this program unique?
1:31 What are some common pediatric surgery cases?
2:23 Explain your work as a pediatric general surgeon?

Pediatric surgeons at Texas Children’s Hospital West Campus perform general surgical procedures such as circumcisions, removal of foreign objects, hernia repair, and suturing of minor lacerations. While more complex surgeries take place at the Texas Children’s Main Campus, pre-operative and follow-up outpatient care for those procedures is available at the West Campus.
Everything about Texas Children’s Hospital West Campus is dedicated to the health and wellness of children. As greater Houston's first suburban hospital designed exclusively for children, we offer the expert care you've come to trust from Texas Children's Hospital coupled with a location that's convenient and accessible for area families. Our facility is located just off the westbound feeder road of the Katy Freeway (at I-10 and Barker Cypress).
For more information about Texas Children's Hospital West Campus, visit http://www.texaschildrens.org/....Locate/In-the-Commun
Meet Dr. Allen Milewicz, chief of community surgery at Texas Children's West Campus
https://www.youtube.com/watch?v=uMoCdipuKfA&index=16&list=PLiN68C9rloPBD-E9ChWhVy73h7V3SEMlm

World-renowned surgeons at Shriners Hospitals for Children – Northern California provide complex pediatric surgery for children one-year and older with congenital and acquired conditions. Children from throughout the Western United States with chest wall malformations, gastro-intestinal disease, ano-rectal disorders, urologic conditions and other complex surgical needs benefit from the expert care. The pediatric surgery team is devoted to the development of innovative and minimally invasive surgical techniques.

MUSC Children’s Health offers South Carolina’s only Level 1 Children’s Surgery Center, representing excellence in inpatient surgery at MUSC Shawn Jenkins Children’s Hospital, as well as outpatient surgery at R. Keith Summey Medical Pavilion. These two state-of-the-art facilities are equipped with a team of pediatric board-certified providers utilizing pediatric-specific devices and the most technologically advanced tools.

Following Dr. Eric Skarsgard on his grueling 19-hour day at BC Children's Hospital, we meet several of his patients -- some of who need surgery that day, and some who have chronic conditions and need regular check-ups with him -- and learn how he works with medical students and on research projects as time allows.
From across the room, using controls and pedals—pediatric surgeons at Golisano Children’s Hospital are now able to operate on patients without even touching them. “It allows performances of deep surgeries in the pelvis or abdomen through tiny, little incisions as opposed to a traditional, large incision to get access to the areas where urologists often operate,” explained Dr. Rahman Abd-El-Barr, a pediatric urologist with Golisano Children’s Hospital of Southwest Florida.
The DaVinci robot is a robotic platform that allows surgeons to do minimally invasive surgery, leaving patients with smaller incisions and a quicker recovery. “This is important because it allows us to minimize recovery time, pain, bleeding with surgery, and especially with kids, it helps them to get back on their feet right away,” he said.
So when high school athlete, Reagan Rebeor found out she needed to have kidney surgery, she decided to have it robotically. “Thankfully, I did that because if not, I would have had a long scar down my stomach instead of small holes, small incisions. I had pain for three days, three or four days. Then after that, I was fine,” she said.
While it’s not an option for all pediatric surgeries, doctors say it can be very beneficial for teenage and adult patients needing reconstructive surgery. An option that allows patients a quicker and easier recovery.
View More Health Matters video segments at LeeHealth.org/Healthmatters/
Lee Health in Fort Myers, FL is the largest network of health care facilities in Southwest Florida and is highly respected for its expertise, innovation and quality of care. For more than 100 years, we’ve been providing our community with personalized preventative health services and primary care to highly specialized care services and robotic assisted surgeries. Lee Health - Caring People. Inspiring Care.
Visit LeeHealth.org

Train with some of the region’s very best pediatric general surgeons — in a two-year, pediatric surgical fellowship training program at Nemours/Alfred I. duPont Hospital for Children. Our hospital’s Division of Pediatric Surgery is offering this program in affiliation with Sidney Kimmel Medical College at Thomas Jefferson University .
The goal of the fellowship is to give individuals who have completed an accredited general surgery residency advanced knowledge and training in the management and surgical treatment of newborns, infants and children.
Our Fellowship Program
This fellowship will help you prepare for certification by the American Board of Surgery, and is accredited by the Accreditation Council for Graduate Medical Education (ACGME).
The Pediatric Surgery Fellowship aims to:
train a well-rounded, empathetic, safe pediatric surgeon who is confident managing all aspects of the surgical care of children.
steward our fellow in quality improvement projects and methodology, and provide research opportunities.
provide a rigorous didactic curriculum for our fellow utilizing 360 degree feedback.
cultivate opportunities for our fellow to educate residents and students.
encourage our fellow to collaborate across specialties.
develop our fellow’s presentation skills during M&M conferences and multi-disciplinary educational meetings.
The program features the full participation of all nine of the pediatric surgical division’s full-time faculty members. Each of these physicians will contribute greatly to your education. Your training will include operating room and outpatient clinic experience, as well as bedside evaluation of children. You’ll also play a role in the organization of formal teaching conferences, held weekly. Formal rotations will be spent on Pediatric Urology, PICU and Neonatology during the first 12 months. The last year will be spent entirely on the Pediatric Surgical Service.
The majority of your inpatient consultative time will take place at Nemours/Alfred I. duPont Hospital for Children, a freestanding children’s hospital in Wilmington, Del. The hospital:
is nationally ranked by U.S. News & World Report in eight pediatric specialties
recently opened expansion with 260 beds
performs more than 2,800 inpatient and 9,300 outpatient surgical procedures each year in our operating rooms
has an on-site delivery center for newborns with complex congenital anomalies
receives more than 50,000 annual visits in our Emergency Department (ED)
is accredited by The American College of Surgeons as a Level One Pediatric Trauma Center
is accredited by the Commission on Accreditation of Rehabilitation Facilities (CARF)
Visit https://www.nemours.org/educat....ion/gme/fellowships/ to learn more.

Female heart surgeons are rare, but pediatric female surgeons are even more so.
Instruments at work, innovation at play. 🔍
Watch on to discover the behind-the-scenes instruments utilised by our NUHCS cardiac surgery expert, A/Prof Theodoros Kofidis, Head of NUHCS' Department of Cardiac, Thoracic & Vascular Surgery (CTVS), for keyhole heart operations. 🔑
To find out more about Minimally Invasive Heart Surgery @ NUHCS, visit: https://[a]www.nuhcs.com.sg%2FOur-Services%2FSpecialties%2FPages%2FMinimally-Invasive-Cardiac-Surgery-Programme.aspx[/a]
Connect with us:
Instagram: @nuhcsofficial
Facebook: www.facebook.com/nuhcs
Website: www.nuhcs.com.sg
LinkedIn: www.linkedin.com/company/nuhcs
To make an appointment with the NUHCS Heart Clinic, email us at appointment@nuhs.edu.sg
#NUHCS #cardiacsurgery #heartsurgery #keyholesurgery #minimallyinvasive

How to Start an IV Like a Pro (Nursing Skills)
Get the full lesson here: https://nursing.com/lesson/ski....lls-02-01-starting-a
FREE Nursing School Cheat Sheets at: http://www.NURSING.com
Welcome to the NURSING Family, we call it the most supportive nursing cohort on the planet.
At NURSING.com, we want to help you remove the stress and overwhelm of nursing school so that you can focus on becoming an amazing nurse.
Check out our freebies and learn more at: (http://www.nursing.com)
In our Nursing Skills course, we show you the most common and most important skills you will use as a nurse! We included everything from bed baths, to inserting a foley, to advanced skills like chest tube management.
How to Start an IV Like a Pro (Nursing Skills):
This video covers the nursing skill of starting an IV. Here are some tips and tricks to hit that vein every time!
Bookmarks:
0:07 Introduction to starting an IV
0:32 First steps/ Locating a good vein
1:03 Preparing supplies
1:59 Tourniquet replacement
2:11 Cleaning the site
2:26 Inspecting the angiocath
2:46 How to insert the angiocath
3:19 Stabilizing the catheter
3:53 Dressing the catheter
4:19 Labeling the dressing
4:25 Sharps and trash disposal
4:34 Closing words of inspiration
Visit us at http://www.nursing.com/medical-inform... for disclaimer information.
NCLEX®, NCLEX-RN® are registered trademarks of the National Council of State Boards of Nursing, INC. and hold no affiliation with NURSING.com.

Ellis demonstrates how to perform a sterile wound dressing change. It would be appropriate to perform hand hygiene between glove changes.
Our Critical Nursing Skills video tutorial series is taught by Ellis Parker MSN, RN-BC, CNE, CHS and intended to help RN and PN nursing students study for your nursing school exams, including the ATI, HESI and NCLEX.
#NCLEX #ClinicalSkills #woundcare #HESI #Kaplan #ATI #NursingSchool #NursingStudent #Nurse #RN #PN #Education #LVN #LPN #nurseeducator
00:00 What to expect
00:51 Prepping for wound dressing change
1:15 Removing the old wound dressing
1:40 Assessing a wound
2:05 Setting up sterile field
2:49 Sterile gloving
4:02 Preparing equipment for wound dressing change
5:09 Cleaning a wound
6:13 Drying a wound
6:28 Packing a wound
7:19 Covering a wound
7:47 Labeling a wound dressing
🚨 Reminder: shipping deadlines are looming 👀
🎁 Regular Shipping: Order by Friday, December 15
🚀 Expedited Shipping: Order by Monday, December 18
🔍 Still searching for last-minute gifts? Consider a Level Up RN Gift Card! 💌 It’s not only a thoughtful present but also the perfect way to share treasures like Pharmacology Flashcards OR digital treasures like Flashables Digital Nursing Flashcards & the Level Up RN membership. Give the gift of knowledge this holiday season! 🧠⚡️💖 bit.ly/LevelUpRNGC
🚪 Access our Cram Courses, Quizzes and Videos all in one ad free space with Level Up RN Membership https://bit.ly/LevelUpRNMembership
Want more ways to MASTER Clinical Skills? Check out our flashcards & videos!
👇👇👇👇👇👇👇👇👇👇
👉 https://bit.ly/clinicalnursingskills 👈
☝️👆☝️👆☝️👆☝️👆☝️👆
This is your one-stop-shop for materials to help you LEARN & REVIEW so you can PASS Nursing School.
🤔🤔🤔 DO YOU WANT TO PASS your classes, proctored exams and the NCLEX? 🤔🤔🤔 Our resources are the best you can buy. They are built with a single goal: help you pass with no fluff. Everything you need, and nothing you don’t. Don’t take our word for it, though! Check out our hundreds of ⭐️⭐️⭐️⭐️⭐️ reviews from nurses who passed their exams and the NCLEX with Level Up RN.
🗂️ Our Ultimate Nursing School Survival kit is your number 1 resource to get through nursing school and to pass the NCLEX. Whether you're just starting school or you’re already prepping for the NCLEX, this bundle of flashcards is the best you can buy. It covers all the information you need to know to pass all your exams and it has FREE shipping!
➡️ https://bit.ly/TUNSSK ⬅️
L👀king for EVEN MORE resources to survive Nursing School? Make your Nursing School experience your own! Life’s difficult enough—learning shouldn’t be.
🪅 Games https://nursesquad.com
💻 Digital resources https://bit.ly/NursingStudyCourses
📅 Organizational tools https://bit.ly/OrganizingSchool
✨Want perks? Join our channel!
https://youtube.com/leveluprn/join
🏷 Head to https://leveluprn.com/specials for all our latest deals!🥳️
📧 LOOKING FOR FREE RESOURCES TO HELP WITH YOUR EXAMS? Get exclusive tips, latest video releases and more delivered to your email!
➡️ https://leveluprn.com/signup ⬅️
⚕ 👩 LEVEL UP NURSE SQUAD 👩⚕️
All of the nurses at Level Up RN are here to help! Cathy Parkes started helping her fellow classmates back when she was in nursing school, tutoring so they could pass their exams and graduate. After she got her BSN and started working as an RN at Scripps Encinitas Hospital, she started this YouTube channel to help nursing students around the world. Since then she has built a team of top-notch dedicated nurses and nurse educators who are focused on improving nursing education and supporting career advancement for nurses everywhere. With flashcards, videos, courses, organizational tools and more, we are singularly focused on helping students and nurses Level Up on their exams and nursing careers.
