- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Watch that Female Recto-vaginal Exam Video
https://www.youtube.com/watch?v=Uc6ZotU5mxA

Normal Vaginal Delivery

ectal exam is an internal examination of the rectum such as by a physician or other healthcare professional.
The digital rectal examination (DRE, Latin palpatio per anum or PPA) is a relatively simple procedure. The patient is placed in a position where the anus is accessible and relaxed (lying on the side, squatting on the examination table, bent over the examination table, etc). The physician inserts a gloved and lubricated finger into the rectum through the anus and palpates the insides.
The DRE is inadequate as a screening tool for colorectal cancer because it examines less than 10% of the colorectal mucosa; colonoscopy is preferred. However, it's an important part of a general examination, as many tumors or other diseases are made manifest in the distal part of the rectum.
This examination may be used: * for the diagnosis of rectal tumors and other forms of cancer; * in males, for the diagnosis of prostatic disorders, notably tumors and benign prostatic hyperplasia; * for the diagnosis of appendicitis or other examples of an acute abdomen (i.e. acute abdominal symptoms indicating a serious underlying disease); * for the estimation of the tonicity of the anal sphincter, which may be useful in case of fecal incontinence or neurologic diseases, including traumatic spinal cord injuries; * in females, for gynecological palpations of internal organs * for examination of the hardness and color of the feces (ie. in cases of constipation, and fecal impaction); * prior to a colonoscopy or proctoscopy. * to evaluate haemorrhoids
The DRE is frequently combined with an FOBT (fecal occult blood test), which may be useful for diagnosing the etiology of an anemia and/or confirming a gastrointestinal bleed.
Sometimes proctoscopy may also be part of a rectal examination.

http://www.proctoscopeexam.com This is a demonstration of a proctoscope examination of the rectum.

http://www.hypodermic-injection.com This is a demonstration of an IM hypodermic injection administered in the gluteus maximus muscle. The patient is in the prone position.

Abortion real ghraphics

Visit our website to learn more about using Nucleus content for patient engagement and content marketing: http://www.nucleushealth.com/
#LaparoscopicColectomy #ColonSurgery #LargeIntestine
A colectomy is usually done to treat diseases that inflame your colon, a bowel obstruction, colon cancer, or a damaged or injured colon. The anatomy of the colon, and the laparoscopic procedure done to remove a portion of the colon, are depicted.
ANH18221

Bartholin gland Marsupialization in Primary Bartholin Cyst

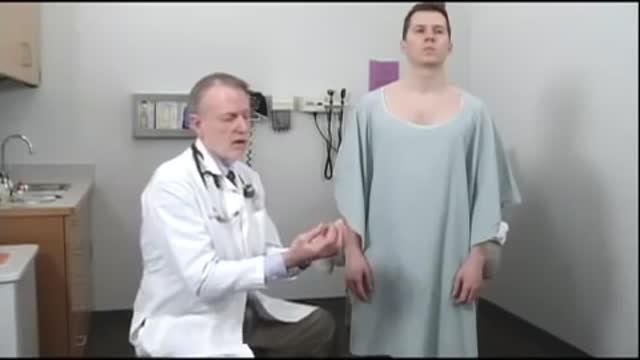
Physical exam by a urologist including kidney, testicular and prostate exam.

In your first few months of pregnancy, hormones flood your body. Your baby is still tiny but already your body is changing. Your breasts start to swell and may feel tender. Tiredness, nausea and frequent trips to the loo are common pregnancy symptoms.

Bandages Different Applications
Vertebrobasilar insufficiency is typically secondary to emboli, thrombi, or arterial dissection. The labyrinth and brainstem are commonly affected, and symptoms may include vertigo, dizziness, dysarthria, diplopia, and numbness.

Pregnancy Tips : How Early Can You Take a Blood Test for Pregnancy?
-Osler-Rendu-Weber syndrome is characterized by multiple telangiectasias and vascular lesions of the CNS.


This video show a lip biopsy on a 38-year old man with a swelling of the lower lip of unknown origin.

Dr Chris Steele demonstrates a breast examination on a live model. This shows how to check yourself for early signs of tumours, cysts and other symptoms of breast cancer.

Early Signs that Cancer is Growing in Your Body

A Cesarean section (C-section) is surgery to deliver a baby. The baby is taken out through the mother's abdomen. In the United States, almost one in three women has their babies this way. Some C-sections are planned, but many are done when unexpected problems happen during delivery. Reasons for a C-section may include Health problems in the mother The mother carrying more than one baby The size or position of the baby The baby's health is in danger Labor is not moving along as it should
