- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

A new procedure helps patients with unattractive bunions and hammertoes.

Lattrell Wells was a perfect candidate for the MACI procedure. Dr. Michael O'Malley is a sports medicine surgeon at Carilion Clinic, "It’s a two stage procedure. So what we do is we actually harvest a small portion of the patient's cartilage and bone cells and we send it to a lab where the lab then that grows additional cartilage cells. It comes back to us in a little sheet and six weeks after that initial surgery, we re-implant the cartilage in a second surgery where we implant that sheet depending on the size of lesion right where his defect. This the only option where there’s virtually no risk of any kind of graft rejection or anything of that nature.

In this video, Dr. Robert Rozbruch, chief of Limb Lengthening and Complex Reconstruction at Hospital for Special Surgery performs an osseointegration after a primary amputation. The patient, a 40 year old woman, had chronic nerve pain and compromised function of her residual limb.
For more information, visit: https://www.limblengthening.com/
https://www.hss.edu/limblengthening
https://www.hss.edu/LSARC
https://www.facebook.com/limblengtheningNYC
https://www.instagram.com/limblengthening
https://www.twitter.com/limblengthen
https://www.youtube.com/channe....l/UC-JL_X6ALjZXiXtcP
key words: Osseointegration, Amputee, Amputation, Limb Replacement, Tibia, Osseointegration

From UW Health's Neurosurgery Program: Learn more about the individual steps in the DBS surgery procedure. Visit uwhealth.org/dbs

If a fetal lung lesion is causing heart failure, fetal surgery may be performed to remove the CCAM before birth. http://fetalsurgery.chop.edu
N. Scott Adzick, MD, Mark Johnson, MD, and Holly Hedrick, MD, experts from the Center for Fetal Diagnosis and Treatment at Children’s Hospital of Philadelphia, explain when fetal intervention for CCAM is recommended, the various approaches that may be used to treat the most complex fetal lung lesions before birth, and how these procedures are performed.
One concern with fetal lung lesions is that they take up space in the chest. If the lung mass grows and pushes the heart and other organs out of place, it can lead to complications such as fetal hydrops (heart failure in the fetus). If this happens, a fetal surgery procedure may be performed to remove the CCAM before birth.
In other cases, an EXIT procedure may be performed to partially deliver the baby, so the team can remove the mass before the baby is fully delivered.
In this video series, parents, nurses and doctors from Children’s Hospital of Philadelphia’s Center for Fetal Diagnosis and Treatment talk about the different types of fetal lung lesions like congenital cystic adenomatoid malformation (CCAM) and bronchopulmonary sequestration (BPS), the importance of accurate diagnosis and monitoring, and the most advanced treatment options currently available. They also discuss follow-up care and long-term outcomes for babies diagnosed with fetal lung lesions.
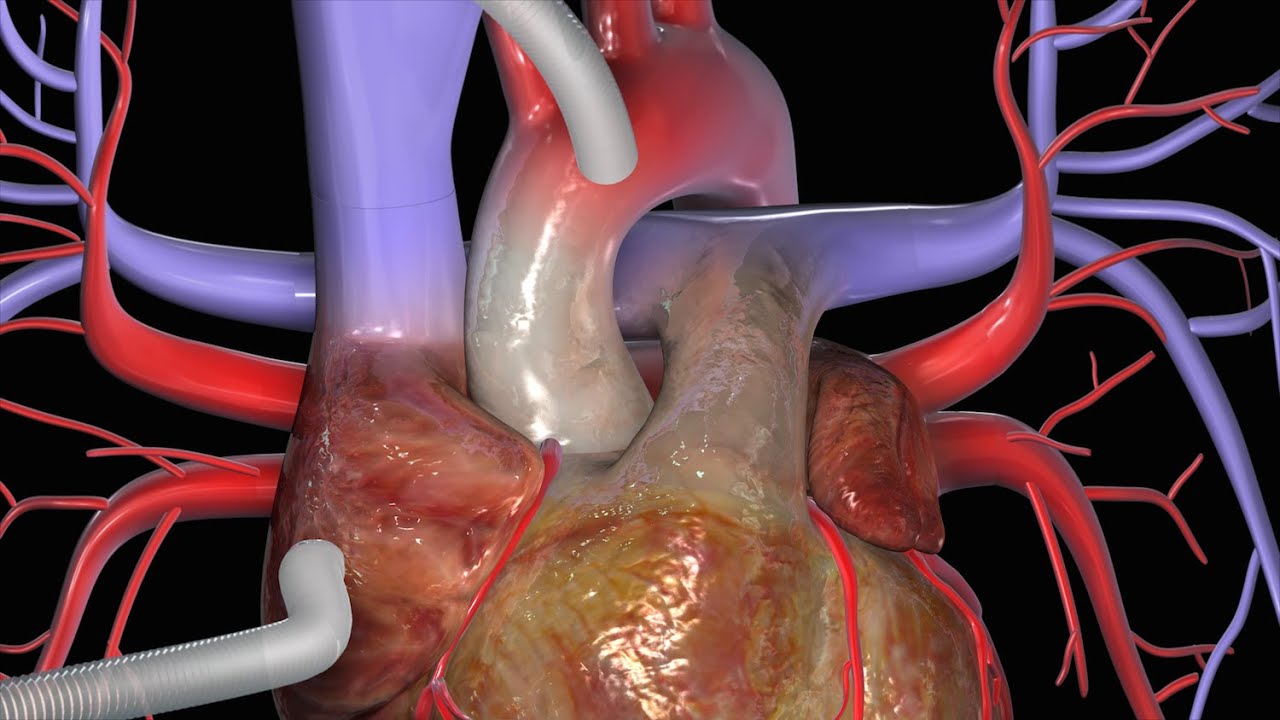
This video has been updated to include an alternate name for the internal thoracic arteries. View the updated video here: https://youtu.be/kxc22Fjd1NQ
For Employees of Hospitals, Schools, Universities and Libraries: Download 8 FREE medical animations from Nucleus by signing up for a free trial: http://nmal.nucleusmedicalmedi....a.com/free-trial-mem
Biology students: Subscribe to the Nucleus Biology channel to see new animations on biology and other science topics, plus short quizzes to ace your next exam: https://bit.ly/3lH1CzV
This video, created by Nucleus Medical Media, shows a coronary artery bypass graft (CABG) procedure used to combat coronary artery disease. Beginning with a midline sternal incision, the heart is connected to a perfusion machine which will take over the duties of the heart while the surgery takes place. Two different grafts are used to bypass the blocked coronary arteries: the internal thoracic artery from inside the chest wall, and the saphenous vein from the leg. After the procedure, the heart is shocked to restart its beating. A drainage tube is left at the incision site to drain away excess fluid. The animation continues to show two other types of approaches to a coronary artery bypass graft, off-pump bypass surgery and minimally invasive bypass surgery.
This is similar to the procedure performed on former president Bill Clinton and former California governor Arnold Schwarzenegger.
#HeartBypassSurgery #CABG #heart
ANCE00199

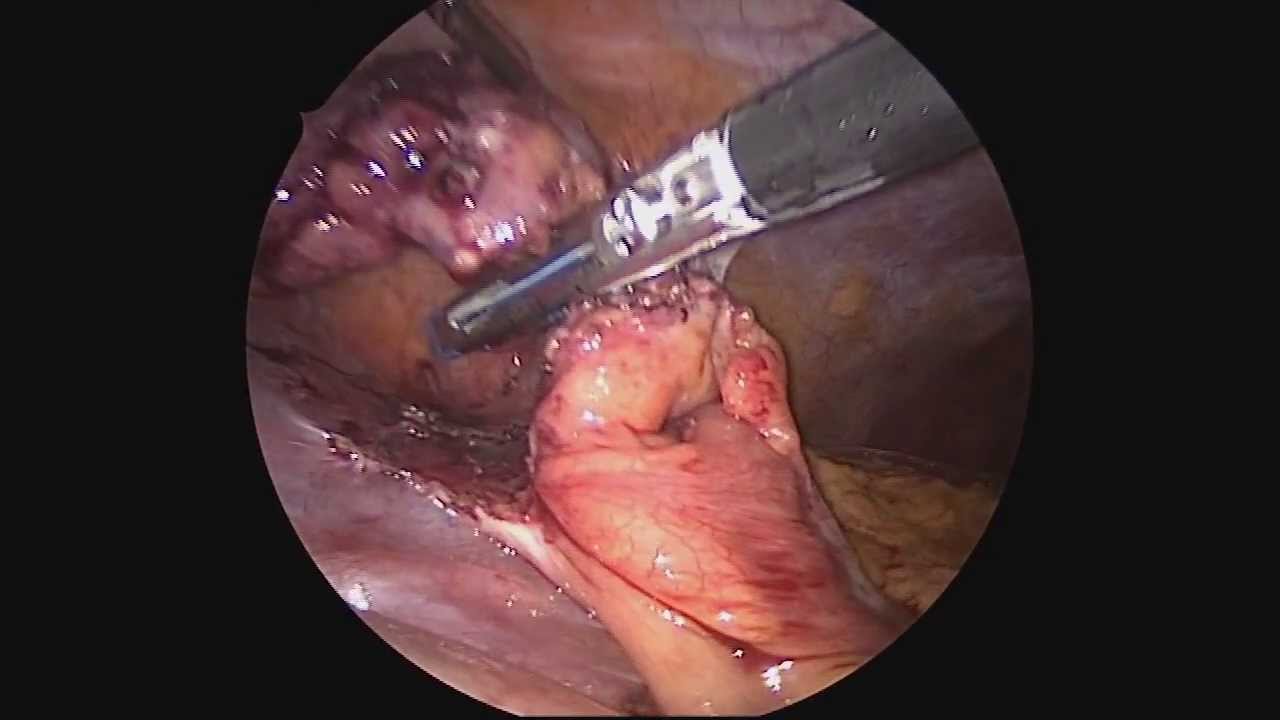
Learn Basic Laparoscopic Surgery, the components of a laparoscopic surgical setup, optimal positioning and ergonomics in laparoscopic surgery, and much more. Check out the full course for free here: https://www.incision.care/free-trial
What is Laparoscopic Surgery:
Laparoscopic surgery describes procedures performed using one or multiple small incisions in the abdominal wall in contrast to the larger, normally singular incision of laparotomy. The technique is based around principles of minimally invasive surgery (or minimal access surgery): a large group of modern surgical procedures carried out by entering the body with the smallest possible damage to tissues. In abdominopelvic surgery, minimally invasive surgery is generally treated as synonymous with laparoscopic surgery as are procedures not technically within the peritoneal cavity, such as totally extraperitoneal hernia repair, or extending beyond the abdomen, such as thoraco-laparoscopic esophagectomy. The term laparoscopy is sometimes used interchangeably, although this is often reserved to describe a visual examination of the peritoneal cavity or the purely scopic component of a laparoscopic procedure. The colloquial keyhole surgery is common in non-medical usage.
Surgical Objective of Laparoscopic Surgery:
The objective of a laparoscopic approach is to minimize surgical trauma when operating on abdominal or pelvic structures. When correctly indicated and performed, this can result in smaller scars, reduced postoperative morbidity, shorter inpatient durations, and a faster return to normal activity. For a number of abdominopelvic procedures, a laparoscopic approach is now generally considered to be the gold-standard treatment option.
Definitions
Developments of Laparoscopic Surgery:
Following a number of smaller-scale applications of minimally invasive techniques to abdominopelvic surgery, laparoscopic surgery became a major part of general surgical practice with the introduction of laparoscopic cholecystectomy in the 1980s and the subsequent pioneering of endoscopic camera technology. This led to the widespread adoption of the technique by the early- to mid-1990s. The portfolio of procedures that can be performed laparoscopically has rapidly expanded with improvements in instruments, imaging, techniques and training — forming a central component of modern surgical practice and cross-specialty curricula [2]. Techniques such as laparoscopically assisted surgery and hand-assisted laparoscopic surgery have allowed the application of laparoscopic techniques to a greater variety of pathology. Single-incision laparoscopic surgery, natural orifice transluminal endoscopic surgery, and minilaparoscopy-assisted natural orifice surgery continue to push forward the applications of minimally invasive abdominopelvic techniques; however, the widespread practice and specific indications for these remain to be fully established. More recently, robotic surgery has been able to build on laparoscopic principles through developments in visualization, ergonomics, and instrumentation.
This Basic Laparoscopic Surgery Course Will Teach You:
- Abdominal access techniques and the different ways of establishing a pneumoperitoneum
- Principles of port placement and organization of the operative field
- Key elements of laparoscopic suturing, basic knotting and clip application
Specific attention is paid to the following hazards you may encounter:
- Fire hazard and thermal injury
- Lens fogging
- Contamination of insufflation system
- Complications from trocar introduction
- Limitations of Veress needle technique
- Limitations of open introduction technique
- Complications of the pneumoperitoneum
- Gas embolism
- Mirroring and scaling of instrument movements
- Firing clip applier without a loaded clip
The following tips are designed to improve your understanding and performance:
- Anatomy of a laparoscope
- Checking for optic fiber damage
- "White balance" of camera
- Checking integrity of electrosurgical insulation
- Access at Palmer's point
- Lifting abdominal wall before introduction
- Confirming position of Veress needle
- Umbilical anatomy
- Identification of inferior epigastric vessels under direct vision
- Translumination of superficial epigastric vessels
- Selection of trocar size
- Aiming of trocar
- Working angles in laparoscopic surgery
- Choice of suture material
- Instruments for suturing
- Optimal ergonomics for suturing
- Extracorporeal needle positioning
- Optimal suture lengths
- "Backloading" needle
- Intracorporeal needle positioning
- Hand movements when suturing
- Optimal positioning of scissors
- Extracorporeal knot tying
- Visualization of clip applier around target structure
- Common clip configurations

Mini-Laparoscopic Cholecystectomy with Intraoperative Cholangiogram for Symptomatic Cholelithiasis (Gallstones) - Extended
Authors: Brunt LM1, Singh R1, Yee A2
Published: September 26, 2017
AUTHOR INFORMATION
1 Department of Surgery, Washington University, St. Louis, Missouri
2 Division of Plastic and Reconstructive Surgery, Washington University, St. Louis, Missouri
DISCLOSURE
No authors have a financial interest in any of the products, devices, or drugs mentioned in this production or publication.
ABSTRACT
Minimal invasive laparoscopic cholecystectomy is the typical surgical treatment for cholelithiasis (gallstones), where patients present with a history of upper abdominal pain and episodes of biliary colic. The classic technique for minimal invasive laparoscopic cholecystectomy involves four ports: one umbilicus port, two subcostal ports, and a single epigastric port. The Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) has instituted a six-step strategy to foster a universal culture of safety for cholecystectomy and minimize risk of bile duct injury. The technical steps are documented within the context of the surgical video for (1) achieving a critical view of safety for identification of the cystic duct and artery, (2) intraoperative time-out prior to management of the ductal structures, (3) recognizing the zone of significant risk of injury, and (4) routine intraoperative cholangiography for imaging of the biliary tree. In this case, the patient presented with symptomatic biliary colic due to a gallstone seen on the ultrasound in the gallbladder. The patient was managed a mini-laparoscopic cholecystectomy using 3mm ports for the epigastric and subcostal port sites with intraoperative fluoroscopic cholangiogram. Specifically, the senior author encountered a tight cystic duct preventing the insertion of the cholangiocatheter and the surgical video describes how the author managed the cystic duct for achieving a cholangiogram, in addition to the entire technical details of laparoscopic cholecystectomy.

http://www.amerra.com In this patient education video from Colorectal Surgical Associates in Houston, Texas, learn more about the single incision laparoscopic colectomy procedure. This minimally invasive procedure uses a mini incision that
results in less pain, fewer complications, earlier recovery, and a smaller scar. Colorectal cancer is the second leading cause of cancer death in the United States. For more information please visit our website: www.csamd.com or call (713)-790-0600.

.
Chapters
0:00 Introduction
1:04 Why do doctors perform laparoscopy?
2:11 How is laparoscopy performed?
3:22 Result
3:47 Risk of laparoscopy
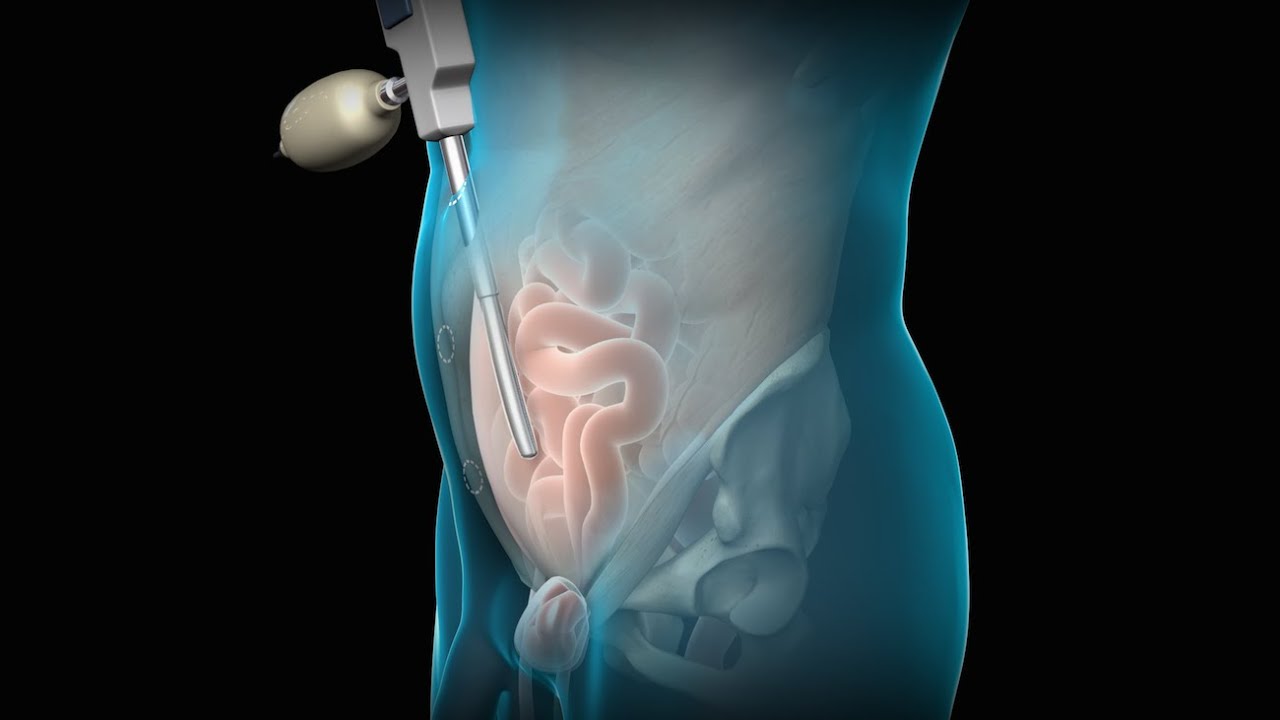
Laparoscopy (from Ancient Greek λαπάρα (lapára) 'flank, side', and σκοπέω (skopéō) 'to see') is an operation performed in the abdomen or pelvis using small incisions (usually 0.5–1.5 cm) with the aid of a camera. The laparoscope aids diagnosis or therapeutic interventions with a few small cuts in the abdomen.[1]
Laparoscopic surgery, also called minimally invasive procedure, bandaid surgery, or keyhole surgery, is a modern surgical technique. There are a number of advantages to the patient with laparoscopic surgery versus an exploratory laparotomy. These include reduced pain due to smaller incisions, reduced hemorrhaging, and shorter recovery time. The key element is the use of a laparoscope, a long fiber optic cable system that allows viewing of the affected area by snaking the cable from a more distant, but more easily accessible location.
Laparoscopic surgery includes operations within the abdominal or pelvic cavities, whereas keyhole surgery performed on the thoracic or chest cavity is called thoracoscopic surgery. Specific surgical instruments used in laparoscopic surgery include obstetrical forceps, scissors, probes, dissectors, hooks, and retractors. Laparoscopic and thoracoscopic surgery belong to the broader field of endoscopy. The first laparoscopic procedure was performed by German surgeon Georg Kelling in 1901. There are two types of laparoscope:[2]
A telescopic rod lens system, usually connected to a video camera (single-chip or three-chip)
A digital laparoscope where a miniature digital video camera is placed at the end of the laparoscope, eliminating the rod lens system
The mechanism mentioned in the second type is mainly used to improve the image quality of flexible endoscopes, replacing conventional fiberscopes. Nevertheless, laparoscopes are rigid endoscopes. Rigidity is required in clinical practice. The rod-lens-based laparoscopes dominate overwhelmingly in practice, due to their fine optical resolution (50 µm typically, dependent on the aperture size used in the objective lens), and the image quality can be better than that of the digital camera if necessary. The second type of laparoscope is very rare in the laparoscope market and in hospitals.[citation needed]
Also attached is a fiber optic cable system connected to a "cold" light source (halogen or xenon) to illuminate the operative field, which is inserted through a 5 mm or 10 mm cannula or trocar. The abdomen is usually insufflated with carbon dioxide gas. This elevates the abdominal wall above the internal organs to create a working and viewing space. CO2 is used because it is common to the human body and can be absorbed by tissue and removed by the respiratory system. It is also non-flammable, which is important because electrosurgical devices are commonly used in laparoscopic procedures.[3]
Procedures
Surgeons perform laparoscopic stomach surgery.
Patient position
During the laparoscopic procedure, the position of the patient is either in Trendelenburg position or in reverse Trendelenburg. These positions have an effect on cardiopulmonary function. In Trendelenburg's position, there is an increased preload due to an increase in the venous return from lower extremities. This position results in cephalic shifting of the viscera, which accentuates the pressure on the diaphragm. In the case of reverse Trendelenburg position, pulmonary function tends to improve as there is a caudal shifting of viscera, which improves tidal volume by a decrease in the pressure on the diaphragm. This position also decreases the preload on the heart and causes a decrease in the venous return leading to hypotension. The pooling of blood in the lower extremities increases the stasis and predisposes the patient to develop deep vein thrombosis (DVT).[4]
Gallbladder
Rather than a minimum 20 cm incision as in traditional (open) cholecystectomy, four incisions of 0.5–1.0 cm, or more recently, a single incision of 1.5–2.0 cm,[5] will be sufficient to perform a laparoscopic removal of a gallbladder. Since the gallbladder is similar to a small balloon that stores and releases bile, it can usually be removed from the abdomen by suctioning out the bile and then removing the deflated gallbladder through the 1 cm incision at the patient's navel. The length of postoperative stay in the hospital is minimal, and same-day discharges are possible in cases of early morning procedures.[citation needed]
Colon and kidney
Dr. Celia Divino, Chief, Division of General Surgery at The Mount Sinai Hospital, performs a laparoscopic appendectomy. Visit the Division of General Surgery at http://bit.ly/18z944M. Click here to learn more about Dr. Celia Divino http://bit.ly/12RF0ee

OB_A_1013
3D animation depicting the operating room and initial procedure preparing the patient for a laparoscopic hysterectomy. The patient is prepped and draped in the usual fashion and surrounded by the surgeon and surgical assistants. The skin is elevated, an infraumbilical incision is made, a trocar port is inserted through the incision and the abdomen is insufflated. Finally, a laparoscope is inserted into the port to allow for direct visualization of the uterus and the surgery can begin.
To view more animations and exhibits, visit our medical library: https://www.trialexhibitsinc.c....om/library/multimedi
Contact us on your next case for consulting, trial graphics, animations, medical illustrations or presentation services. 800-591-1123 [a]www.trialex.com[/a]
This video is for reference only. The video may not be otherwise used, reproduced nor modified. For more information to purchase a copy or permission to use this animation on your next case, project, website or TV, contact us at [a]www.trialex.com[/a] or 800-591-1123.
Copyright @ Trial Exhibits, Inc.

UChicago Medicine organ transplant surgeon Dr. Rolf Barth explains a how the laparoscopic donor nephrectomy – also known as the single-port nephrectomy – procedure works to remove an organ donor’s kidney from their body to be transplanted into a recipient. This minimally invasive kidney donor transplant surgery allows living organ donors the get back to their lives more quickly than the traditional approach and leaves them with a nearly invisible scar in the belly button.
Learn more about living kidney donation: https://www.uchicagomedicine.o....rg/conditions-servic
To license this video for patient education or content marketing, visit: http://www.nucleushealth.com/?utm_source=youtube&utm_medium=video-description&utm_campaign=tephernia-030615
An inguinal hernia is a bulging of the intestine through a defect or weak spot in the wall of the lower abdomen. This video shows how inguinal hernias form and how they are treated.
#TotalExtraperitonealLaparoscopicInguinalHerniaRepair #TEP #laparoscopy
ANCE00200

Visit our website to learn more about using Nucleus content for patient engagement and content marketing: http://www.nucleushealth.com/
#LaparoscopicColectomy #ColonSurgery #LargeIntestine
A colectomy is usually done to treat diseases that inflame your colon, a bowel obstruction, colon cancer, or a damaged or injured colon. The anatomy of the colon, and the laparoscopic procedure done to remove a portion of the colon, are depicted.
ANH18221

Laparoscopic surgery is minimally-invasive (keyhole) surgery and it is performed through very small incisions, using a camera to guide the surgeon during the procedure. Miss Sarah Mills, a top colorectal surgeon, explains why laparoscopic surgery is performed over alternative methods.
Make an appointment with Miss Sarah Mills here: https://www.topdoctors.co.uk/doctor/sarah-mills

Vatche, Minassian, MD, MPH, Chief of Urogynecology, and Sarah Cohen, MD, MPH, Director of the Minimally Invasive Gynecologic Surgery Fellowship Program at Brigham and Women’s Hospital, perform a laparoscopic burch colposuspension, a procedure used to correct stress urinary incontinence.
Stress urinary incontinence is one of the most common types of incontinence and is characterized by urinary leakage during physical activities including coughing, sneezing, exercising, lifting, and laughing. As the condition progresses, it can become severe enough to happen with simple acts such as bending and walking. This condition is due to an anatomic weakness of the bladder neck which typically maintains the seal of urine during activity. Stress incontinence can result from a variety of conditions including vaginal childbirth, aging, menopause and obesity. As this is an anatomic condition, primary treatment may involve pelvic floor exercises and/or minimally invasive surgery.
Learn more about treatment for stress urinary incontinence:
Division of Urogynecology: http://www.brighamandwomens.or....g/Departments_and_Se
Division of Minimally Invasive Gynecologic Surgery: http://www.brighamandwomens.or....g/Departments_and_Se

For more videos, please visit:
http://surgicalfilmatlas.mssm.edu/


Dr. Erica Hodgman discusses pediatric surgery at the Johns Hopkins Children's Center Pediatric General Surgery program, what common surgeries the program specializes in, what makes the program unique and her work as a pediatric surgeon. #PediatricSurgery #JohnsHopkinsChildrenCenter
Questions Answered:
0:03 Describe the pediatric general surgery division at Johns Hopkins Children's Center.
1:00 What makes this program unique?
1:31 What are some common pediatric surgery cases?
2:23 Explain your work as a pediatric general surgeon?
