- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Have you ever wondered if your toothbrush bristles are too hard or soft or whether or not it even mattered? Contrary to popular belief, the extra soft or soft bristle option is the best choice you can make when it comes to selecting your bristle. The soft bristles are gentler on the gums and because of their delicate nature, it’s easier for them to glide in between teeth. Using hard or medium bristles increases your risk of receding gums and also heightens tooth sensitivity, since you are wearing down the enamel on your teeth with the rough nature. Schedule a dental appointment now to learn more! visit : https://www.urbndental.com/
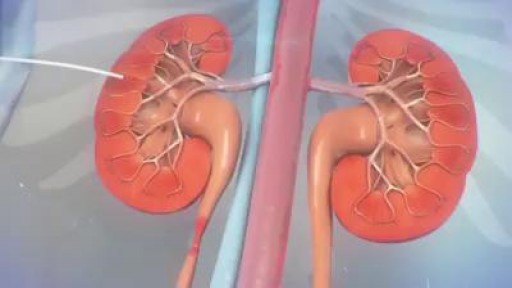
The ureter can become obstructed due to conditions such as kidney stones, tumors, infection, or blood clots. When this happens, physicians can use image guidance to place stents or tubes in the ureter to restore the flow of urine to the bladder. A ureteral stent is a thin, flexible tube threaded into the ureter.

Tonsil Stone Removal with New Tools

In most cases, your body's immune system defeats an HPV infection before it creates warts. When warts do appear, they vary in appearance depending on which variety of HPV is involved: Genital warts. These appear as flat lesions, small cauliflower-like bumps or tiny stem-like protrusions. In women, genital warts appear mostly on the vulva but can also occur near the anus, on the cervix or in the vagina. In men, genital warts appear on the penis and scrotum or around the anus. Genital warts rarely cause discomfort or pain, though they may itch. Common warts. Common warts appear as rough, raised bumps and usually occur on the hands, fingers or elbows. In most cases, common warts are simply unsightly, but they can also be painful or susceptible to injury or bleeding.
Artificial womb could allow babies to develop outside the mother’s uterus
Atrial flutter is a type of abnormal heart rate, or arrhythmia. It occurs when the upper chambers of your heart beat too fast. When the chambers in the top of your heart (atria) beat faster than the bottom ones (ventricles), it complicates your heart rhythm
Politeal and Peroneal Nerves Block

Marfan syndrome is a genetic disorder that affects the body's connective tissue. Connective tissue holds all the body's cells, organs and tissue together. It also plays an important role in helping the body grow and develop properly. Connective tissue is made up of proteins.
As the liver becomes more severely damaged, more obvious and serious symptoms can develop, such as: yellowing of the skin and whites of the eyes (jaundice) swelling in the legs, ankles and feet, due to a build-up of fluid (oedema) swelling in your abdomen, due to a build-up of fluid known as ascites.
Gynecomastia 3D Animation

Sialadenitis is an infection of the salivary glands. It is usually caused by a virus or bacteria . The parotid (in front of the ear) and submandibular (under the chin) glands are most commonly affected. Sialadenitis may be associated with pain, tenderness, redness, and gradual, localized swelling of the affected area.
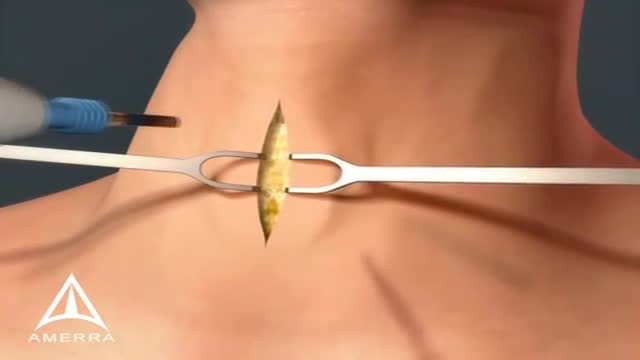
A tracheotomy or a tracheostomy: is simply an opening surgically created through the neck into the trachea (windpipe) to allow direct access to the breathing tube and is commonly done in an operating room under general anesthesia. A tube is usually placed through this opening to provide an airway and to remove secretions from the lungs. Breathing is done through the tracheostomy tube rather than through the nose and mouth. The term “tracheotomy” refers to the incision into the trachea (windpipe) that forms a temporary or permanent opening, which is called a “tracheostomy,” however; the terms are sometimes used interchangeably.
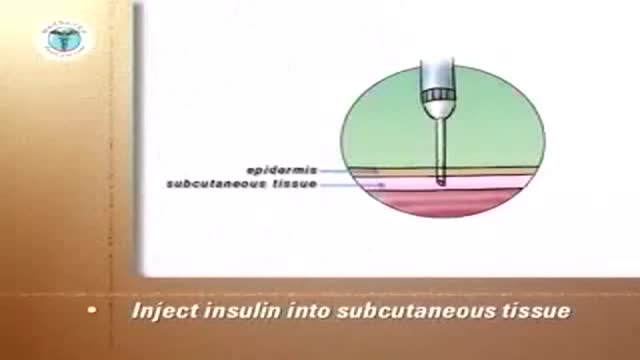
Insulin Pen

Baby born in amniotic sac

Histology of Neurovascular Bundle
Clonidine lowers blood pressure by decreasing the levels of certain chemicals in your blood. This allows your blood vessels to relax and your heart to beat more slowly and easily. The Catapres brand of clonidine is used to treat hypertension (high blood pressure). The Kapvay brand is used to treat attention deficit hyperactivity disorder (ADHD). Clonidine is sometimes given with other medications

A new well designed randomized study has suggested that long term baby aspirin usage may aid in fight against cancer. The suggested mechanism is that cancers induce inflammatory responses so the anti-inflammatory mechanism of prostaglandins inhibitors may cease the progress of many cancers. There are some concerns about the study because despite the well-designed randomized study; the study didn't include a satisfying number of female participants. The study was also conducted on esophageal, colorectal and lung cancers.
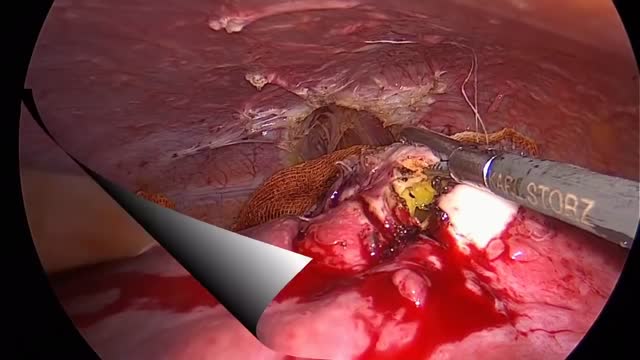
, Liver hydatid cysts of the liver was treated with laparoscopic intervantion . The cysts was located in the eight segment of the liver.
![So You Want to Be a CARDIOTHORACIC SURGEON [Ep. 13]](https://i.ytimg.com/vi/sdxz242qDFA/maxresdefault.jpg)
So you want to be a cardiothoracic surgeon. You like the idea of open heart surgery and the glory that comes with being a CT surgeon. Let’s debunk the public perception myths of what it means to be a cardiothoracic surgeon, and give it to you straight. This is the reality of cardiothoracic surgery.
✒️ Accompanying Blog Post: https://medschoolinsiders.com/....medical-student/so-y
💌 Sign up for my weekly newsletter - https://medschoolinsiders.com/newsletter
🌍 Website & blog - https://medschoolinsiders.com
📸 Instagram - https://instagram.com/medschoolinsiders
🐦 Twitter - https://twitter.com/medinsiders
🗣️ Facebook - https://facebook.com/medschoolinsiders
🎥 My Youtube Gear: https://kit.co/kevinjubbalmd/
👀 Hand Picked Productivity Tools: https://www.amazon.com/shop/medschoolinsiders
🎵My Study Playlist: https://open.spotify.com/user/....1231934998/playlist/
TIME STAMPS:
00:41 - What is Cardiothoracic Surgery?
04:08 - How to Become a Cardiothoracic Surgeon
06:29 - Subspecialties within Cardiothoracic Surgery
07:49 - What You’ll Love About Cardiothoracic Surgery
09:10 - What You Won’t Love About Cardiothoracic Surgery
10:04 - Should You Become a Cardiothoracic Surgeon?
LINKS FROM VIDEO:
So You Want to Be Playlist: https://www.youtube.com/playli....st?list=PL2ADAFpTg5a
Day in the Life Playlist: https://www.youtube.com/playli....st?list=PLTCN43UFAlB
#medicalschool #cardiothoracicsurgery #soyouwanttobe
====================
Disclaimer: Content of this video is my opinion and does not constitute medical advice. The content and associated links provide general information for general educational purposes only. Use of this information is strictly at your own risk. Kevin Jubbal, M.D. and Med School Insiders LLC will not assume any liability for direct or indirect losses or damages that may result from the use of information contained in this video including but not limited to economic loss, injury, illness or death. May include affiliate links to Amazon. As an Amazon Associate, I may earn a commission on qualifying purchases made through them (at no extra cost to you).

A video showing squared notch
