- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

For more videos, please visit:
http://surgicalfilmatlas.mssm.edu/

This video demonstrate Bilateral Salpingectomy for a patient suffering from hematosalpinx of one side and Hydrosalpinx other side in which one IVF has failed. Laparoscopic salpingectomy. In this less-invasive procedure, the surgeon makes 1-3 small incisions in the lower abdomen, and inserts a laparoscope into the pelvis through one of the incisions. The camera at the end of the laparoscope guides the surgeon through the procedure. The fallopian tube tissue is then removed. For more information https://www.laparoscopyhospital.com/
For more information please contact:
World Laparoscopy Hospital
Cyber City, Gurugram, NCR DELHI
INDIA 122002
Phone & WhatsApp: +919811416838, + 91 9999677788

This video demonstrates Laparoscopic Cholecystectomy Fully Explained Skin-to-Skin Video with Near Infrared Cholangiography performed by Dr R K Mishra at World Laparoscopy Hospital. A laparoscopic cholecystectomy is a minimally invasive surgical procedure that involves removing the gallbladder. It is typically performed using small incisions in the abdomen, through which a laparoscope (a thin tube with a camera and light) and surgical instruments are inserted. The surgeon uses the laparoscope to visualize the inside of the abdomen and to guide the instruments in removing the gallbladder.
Near-infrared cholangiography is a technique that uses a special camera and fluorescent dye to visualize the bile ducts during surgery. The dye is injected into the cystic duct (the tube that connects the gallbladder to the bile ducts) and the camera detects the fluorescence emitted by the dye, allowing the surgeon to see the bile ducts more clearly.
The combination of laparoscopic cholecystectomy and near-infrared cholangiography has become a standard of care in many hospitals and surgical centers. It allows for a more precise and efficient surgery, reducing the risk of complications such as bile duct injury.
The use of indocyanine green (ICG) with near-infrared imaging during laparoscopic cholecystectomy has several advantages. Here are some of them:
Better visualization of the biliary anatomy: ICG with near-infrared imaging allows for better visualization of the biliary anatomy during surgery. This helps the surgeon identify important structures, such as the cystic duct and the common bile duct, and avoid injuring them.
Reduced risk of bile duct injury: With better visualization of the biliary anatomy, the risk of bile duct injury during surgery is reduced. Bile duct injury is a serious complication that can occur during laparoscopic cholecystectomy and can lead to long-term health problems.
Improved surgical precision: ICG with near-infrared imaging also improves surgical precision. The surgeon can better see the tissues and structures being operated on, which can help reduce the risk of bleeding and other complications.
Shorter operating time: The use of ICG with near-infrared imaging can shorten the operating time for laparoscopic cholecystectomy. This is because the surgeon can more quickly and accurately identify the biliary anatomy, which can help streamline the surgery.
Overall, the use of ICG with near-infrared imaging is a valuable tool in laparoscopic cholecystectomy that can improve surgical outcomes and reduce the risk of complications.
Like any surgical procedure, laparoscopic cholecystectomy (gallbladder removal) has potential complications. Here are some of the most common ones:
Bleeding: Bleeding during or after the surgery is a possible complication of laparoscopic cholecystectomy. Most cases are minor and can be easily controlled, but in rare cases, significant bleeding may require a blood transfusion or even additional surgery.
Infection: Any surgical procedure carries a risk of infection. After laparoscopic cholecystectomy, there is a risk of infection at the site of the incisions or within the abdomen. Symptoms may include fever, pain, redness, or drainage from the incision sites.
Bile leakage: In some cases, a small amount of bile may leak from the bile ducts into the abdominal cavity after gallbladder removal. This can cause abdominal pain, fever, and sometimes requires further surgery or treatment.
Injury to nearby organs: During the surgery, there is a small risk of unintentional injury to nearby organs such as the liver, intestines, or bile ducts. This can cause additional complications and may require further treatment.
Adverse reactions to anesthesia: As with any surgery requiring general anesthesia, there is a small risk of adverse reactions to the anesthesia, such as an allergic reaction, respiratory problems, or heart complications.
Most patients recover without complications following a laparoscopic cholecystectomy, but it is important to discuss any concerns or questions with your surgeon beforehand.
Contact us
World Laparoscopy Hospital
Cyber City, Gurugram, NCR Delhi
INDIA : +919811416838
World Laparoscopy Training Institute
Bld.No: 27, DHCC, Dubai
UAE : +971525857874
World Laparoscopy Training Institute
8320 Inv Dr, Tallahassee, Florida
USA : +1 321 250 7653
Regenerate response

Dr. Lohith U, Consultant Surgical Gastroenterology, Bariatric and GI Oncology, Manipal Hospital Sarjapur, speaks about advanced laparoscopic surgery in this informative video. He shares details about the procedure,insights on its advantages, and how it can help treat gastrointestinal issues without making large incisions in a patient’s body. To know more watch this video.
Consult the experts here - https://bit.ly/3RiWqPr
#ManipalHospitalSarjapur #YourManipal #LifesOn #Healthcare #LaparoscopicSurgery

UPMC liver surgeons are among the most experienced in the world in performing minimally invasive liver surgery. Most patients benefit from less trauma and pain, minimal scarring, a shorter hospital stay, and faster recovery than from traditional surgery.
To learn more, please visit https://www.upmc.com/services/....liver-cancer/treatme

Dr. Shaun Kunisaki is an Associate Professor of Surgery at The Johns Hopkins University and Associate Chief of Strategy and Integration in the Division of General Pediatric Surgery at the Johns Hopkins Children's Center. His clinical practice spans the full breadth of pediatric general surgery, but he is recognized both regionally and nationally for this expertise in complex thoracic surgical problems in the fetus and young child. As Director of Pediatric Esophageal Surgery, he specializes in the management of long-gap esophageal atresia. In this role within the Johns Hopkins Children Center Fetal Program, he helps counsel parents with pregnancies complicated by fetal anomalies.
Learn more about Dr. Kunisaki at https://www.hopkinsmedicine.or....g/profiles/results/d

James Dunn, MD, PhD is a pediatric surgeon at Stanford Children's Health. He is board certified in General Surgery and Pediatric Surgery.
Learn more at https://www.stanfordchildrens.....org/en/service/gener

When your child needs surgery, it can be overwhelming and sometimes scary. At Mayo Clinic Children’s Center, our highly skilled surgeons apply deep experience and specialized training to offer individualized care for your child and your family.

MUSC Children’s Health offers South Carolina’s only Level 1 Children’s Surgery Center, representing excellence in inpatient surgery at MUSC Shawn Jenkins Children’s Hospital, as well as outpatient surgery at R. Keith Summey Medical Pavilion. These two state-of-the-art facilities are equipped with a team of pediatric board-certified providers utilizing pediatric-specific devices and the most technologically advanced tools.

If you have an upcoming procedure at UC Davis Children’s Surgery Center, this video provides information and details of what you and your family can expect from arrival to check-in through to surgery and after care.
This video is also available in these languages:
Arabic: https://youtu.be/ERPikb0prlI
Dari: https://youtu.be/UW5fT433IGQ
Punjabi: https://youtu.be/Xq6PV2qtOMo
Russian: https://youtu.be/v223nDdN1b4
Spanish: https://youtu.be/4Jr4dkzAaWA
——
At UC Davis Children’s Hospital, we put your child at the center of everything that we do. It’s personalized care, uniquely sized for your child. You’ll see it in our child-friendly designs throughout the hospital, our farm-to-fork approach to dining, our playrooms and teen rooms and our team that feels like family. UC Davis Children’s Hospital is Sacramento’s only nationally ranked, comprehensive hospital for children, serving infants, children, adolescents and young adults with primary, subspecialty and critical care.
UC Davis Children’s Hospital: https://children.ucdavis.edu
Children’s Surgery Center: https://health.ucdavis.edu/chi....ldren/services/child
Child Life and Creative Arts Therapy: https://health.ucdavis.edu/chi....ldren/services/child
Fetal Care and Treatment Center: https://health.ucdavis.edu/chi....ldren/services/fetal
See the latest news from UC Davis Health: https://health.ucdavis.edu/newsroom
Kids Considered podcast: https://www.youtube.com/playli....st?list=PLM7qvIv8N9R
Facebook: https://www.facebook.com/UCDavisChildrensHospital
Instagram: https://www.instagram.com/ucdavischildren
Twitter/X: https://twitter.com/UCDavisChildren
——
#surgery #childrenshospital #surgeryrecovery #ucdavis

For more than 25 years, The Children's Hospital of Philadelphia — the first Level 1 Pediatric Trauma Center in Pennsylvania — has provided unparalleled medical and surgical care for all injured children, including those with the most severe injuries.
Learn what makes the Trauma Center at CHOP a Level 1 Pediatric Trauma Center, and how our work toward trauma prevention, research advances and overall trauma awareness provides hope for reduced injuries in the future.
Learn more about the Trauma Center at CHOP: http://www.chop.edu/trauma.

Funny Video from hospital waiting room

To save humanity, a dietitian travels to the past. A lot.
Subscribe now: https://www.youtube.com/c/funn....yordie?sub_confirmat
CREDITS:
Director: Elliot Dickerhoof
Producers: Chuck Armstrong, Charlie Stockman, Elliot Dickerhoof
Writers: Chuck Armstrong & Charlie Stockman
Actors: Chuck Armstrong, Charlie Stockman, Kelly Vrooman
Executive Producer: Darren Miller
DP: Cody Jacobs
Gaffer: Jordan Holtane
AC: Giselle Gonzalez
Sound Mixer: Marcos Castro
Costume Designer: Kate Bergh
Hair and Makeup Artist: Jessica Leigh Schwartz
PA: Elyssa Phillips
Get more Funny Or Die
-------------------------------
Like FOD on Facebook: https://www.facebook.com/funnyordie
Follow FOD on Twitter: https://twitter.com/funnyordie
Follow FOD on Tumblr: http://funnyordie.tumblr.com/
Follow FOD on Instagram: http://instagram.com/funnyordie
Follow FOD on Vine: https://vine.co/funnyordie
Follow FOD on Pinterest: http://www.pinterest.com/funnyordie
Follow FOD on Google+: https://plus.google.com/+funnyordie
See the original at: http://www.funnyordie.com/videos/74dd9afee2

While in residency, Marc Pelletier, MD, helped in a bypass surgery and knew it was the field in which he would excel. Watch as the Chief of Cardiac Surgery for University Hospitals Harrington Heart & Vascular Institute in Cleveland, Ohio explains, in detail, what happens in preparation for heart surgery, in the operating room and the feeling he experiences after surgery.
How does a heart-lung machine work? What is 'efficiency of motion'? These questions and more are answered in this compelling, dramatic look at heart surgery.
To learn more about heart surgery at University Hospitals: https://www.uhhospitals.org/fo....r-clinicians/special
University Hospitals is one of the nation’s leading health care systems, providing patient-centered care that meets the highest standards for quality and patient safety and have received numerous awards and recognitions from some of the most prestigious institutions in the country for our leadership and exceptional patient outcomes. As an accountable care organization, we foster long-term patient-provider relationships that help promote preventive care, increase wellness and healthy behaviors, decrease emergency episodes, and prevent hospitalizations. To learn more: https://www.uhhospitals.org

Ever wanted to see an open heart surgery? Dr. Sandwith, the only open-heart surgeon in the tri-county area, takes you into the OR to improve the life of a gentlemen with congenital heart disease.
#HCA_FL #FortWaltonDestinHospital

To learn more about coronary artery bypass grafting (CABG), please visit https://cle.clinic/3b7dqpE
Cardiac surgeons Faisal Baaeen, MD and Edward Soltesz, MD talk about coronary artery bypass graft (CABG) surgery in this informative video.
They describe:
• how blockages are bypassed
• how vessels are used for the bypass graft
• reoperation experiences
• the importance of complete revascularization
• and options such as off pump bypass surgery and minimally invasive surgery
Dr. Bakaeen is the Director of the Coronary Artery Bypass Center at Cleveland Clinic. To learn more about him, please visit https://cle.clinic/2INN9AV
Dr. Soltesz is a cardiovascular and heart transplant surgeon. To learn more about him, please visit https://cle.clinic/3o86RMt
▶Share this video with others: https://youtu.be/Cp59BCMVHHc
▶Subscribe to learn more about @clevelandclinic
#clevelandclinic #coronaryartery #bypasssurgery #heartsurgery #heartcare #cardiacsurgery

Ellis demonstrates how to clean a reusable inner cannula, care for a tracheostomy site, and suction a tracheostomy.
Our Critical Nursing Skills video tutorial series is taught by Ellis Parker MSN, RN-BC, CNE, CHS and intended to help RN and PN nursing students study for your nursing school exams, including the ATI, HESI and NCLEX.
#ClinicalSkills #NCLEX #tracheostomy #patientcare #ATI #Kaplan #LVN #PN #RN #nurseeducator #nurse #nursingstudent #murse #clinicals #clinicalnursingskills
00:00 What to expect Tracheostomy Care and Suctioning
0:33 Explaining the process Tracheostomy Care and Suctioning
1:10 Positioning patient for a Tracheostomy Care and Suctioning
1:33 Opening tray
1:46 Pouring saline
1:58 Removing inner cannula
2:14 Removing clean gloves
2:25 Donning sterile gloves
3:16 Showing tray contents
3:53 Removing previous dressing
4:06 Pouring saline
4:27 Cleaning stoma
5:10 Cleaning faceplate
5:20 Drying site
5:30 Cleaning inner cannula
6:00 Drying inner cannula
6:20 Reinserting inner cannula
6:40 Placing new gauze
7:00 Replacing ties
8:00 Replacing oxygen
8:13 Preparing for suction
8:58 Checking suction
9:30 Opening saline
9:42 Opening kit
9:58 Donning sterile gloves
11:04 Setting up saline container
11:20 Pouring saline
11:52 Connecting catheter to suction
12:46 Inserting catheter
13:10 Removing catheter
13:24 Rinsing catheter
13:40 Reoxyginating
14:05 Reinserting catheter
14:17 Removing catheter
14:29 Rinsing catheter
14:44 Reoxyginating
14:55 Cleaning up
15:09 Chatting about sterility
17:00 Checking a tie
🚨 Reminder: shipping deadlines are looming 👀
🎁 Regular Shipping: Order by Friday, December 15
🚀 Expedited Shipping: Order by Monday, December 18
🔍 Still searching for last-minute gifts? Consider a Level Up RN Gift Card! 💌 It’s not only a thoughtful present but also the perfect way to share treasures like Pharmacology Flashcards OR digital treasures like Flashables Digital Nursing Flashcards & the Level Up RN membership. Give the gift of knowledge this holiday season! 🧠⚡️💖 bit.ly/LevelUpRNGC
🚪 Access our Cram Courses, Quizzes and Videos all in one ad free space with Level Up RN Membership https://bit.ly/LevelUpRNMembership
Want more ways to MASTER Clinical Skills? Check out our flashcards & videos!
👇👇👇👇👇👇👇👇👇👇
👉 https://bit.ly/clinicalnursingskills 👈
☝️👆☝️👆☝️👆☝️👆☝️👆
This is your one-stop-shop for materials to help you LEARN & REVIEW so you can PASS Nursing School.
🤔🤔🤔 DO YOU WANT TO PASS your classes, proctored exams and the NCLEX? 🤔🤔🤔 Our resources are the best you can buy. They are built with a single goal: help you pass with no fluff. Everything you need, and nothing you don’t. Don’t take our word for it, though! Check out our hundreds of ⭐️⭐️⭐️⭐️⭐️ reviews from nurses who passed their exams and the NCLEX with Level Up RN.
🗂️ Our Ultimate Nursing School Survival kit is your number 1 resource to get through nursing school and to pass the NCLEX. Whether you're just starting school or you’re already prepping for the NCLEX, this bundle of flashcards is the best you can buy. It covers all the information you need to know to pass all your exams and it has FREE shipping!
➡️ https://bit.ly/TUNSSK ⬅️
L👀king for EVEN MORE resources to survive Nursing School? Make your Nursing School experience your own! Life’s difficult enough—learning shouldn’t be.
🪅 Games https://nursesquad.com
💻 Digital resources https://bit.ly/NursingStudyCourses
📅 Organizational tools https://bit.ly/OrganizingSchool
✨Want perks? Join our channel!
https://youtube.com/leveluprn/join
🏷 Head to https://leveluprn.com/specials for all our latest deals!🥳️
📧 LOOKING FOR FREE RESOURCES TO HELP WITH YOUR EXAMS? Get exclusive tips, latest video releases and more delivered to your email!
➡️ https://leveluprn.com/signup ⬅️
⚕ 👩 LEVEL UP NURSE SQUAD 👩⚕️
All of the nurses at Level Up RN are here to help! Cathy Parkes started helping her fellow classmates back when she was in nursing school, tutoring so they could pass their exams and graduate. After she got her BSN and started working as an RN at Scripps Encinitas Hospital, she started this YouTube channel to help nursing students around the world. Since then she has built a team of top-notch dedicated nurses and nurse educators who are focused on improving nursing education and supporting career advancement for nurses everywhere. With flashcards, videos, courses, organizational tools and more, we are singularly focused on helping students and nurses Level Up on their exams and nursing careers.
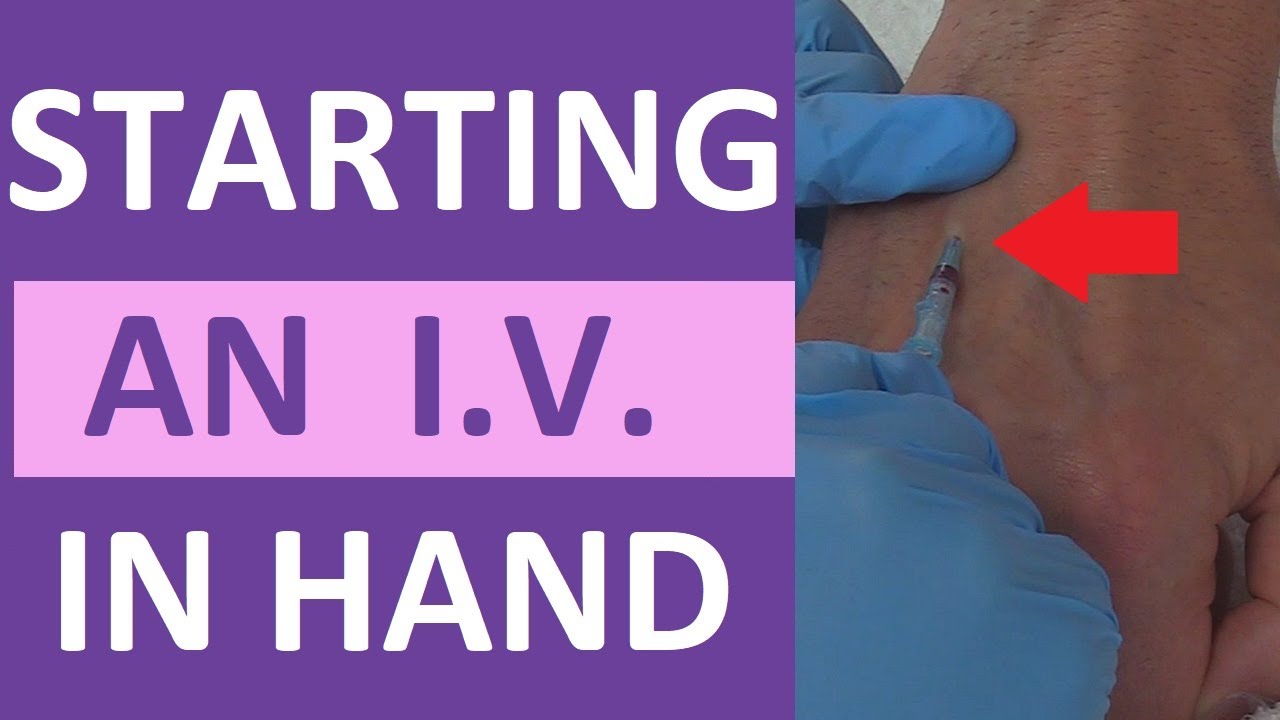
How to start a peripheral IV in the dorsum of the hand: clinical nursing skill technique.
Starting an IV (intravenous catheter) can be an intimidating experience for nurses, especially nursing students and new nurses. However, nurses will perform IV insertions often, so this is an important nursing skill to learn.
Before starting an IV, always follow the protocols of your facility, as well as manufacturer's instructions for any supplies used.
In this video, Nurse Sarah demonstrates how to start a peripheral IV in the dorsum of the hand. Prior to inserting the IV, you'll want to do the following:
-Gather supplies
-Perform hand hygiene
-Prepare supplies (including priming the saline flush, removing air from extension tubing, opening packages, completing labels, and any other steps required by your facility.
-Locate a suitable vein
-Perform hand hygiene
-Don gloves
If the patient has a lot of hair, you might want to use clippers to trim the hairs prior to starting the IV. You may also apply a tourniquet to help veins move near the surface of the skin.
Next, you'll want to clean the site using the cleaner that came in the IV start kit, such as ChloraPrep.
Once the site has dried completely, you can insert the IV. Stabilize the vein with your non-dominant hand, and insert the IV's needle into the vein, watching carefully for blood return (or a blood flash) in the chamber. Advance the IV around 2mm more to ensure the plastic cannula is in the vein, then thread the cannula into the vein and press the needle safety button.
Notes: https://www.registerednursern.....com/how-to-start-an-
IV Video Series: https://www.youtube.com/watch?v=MbG_1-_mnoo&list=PLQrdx7rRsKfXr6kruqEpIovf66sxo0gxh
This video also demonstrates how to flush the IV using the push-pause method, how to secure the IV using the Tegaderm dressing that came with the IV start kit, considerations of the different cap types and the clamp sequence, and more.
For more information, watch the complete tutorial.
#nurse #nursing #iv #startiv #ivtherapy
Website: https://www.registerednursern.com/
More Videos: https://www.youtube.com/watch?v=R2XMro13dD0&list=UUPyMN8DzkFl2__xnTEiGZ1w
Nursing Gear: https://teespring.com/stores/registerednursern
Instagram: https://www.instagram.com/registerednursern_com/
Facebook: https://www.facebook.com/RegisteredNurseRNs
Twitter: https://twitter.com/NursesRN
Popular Playlists:
NCLEX Reviews: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Fluid & Electrolytes: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing Skills: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf

Ellis will be demonstrating how to complete an occupied bed change. It would be appropriate to wear gloves during this skill to avoid contact with bodily fluids.
Our Critical Nursing Skills video tutorial series is taught by Ellis Parker MSN, RN-BC, CNE, CHS and intended to help RN and PN nursing students study for your nursing school exams, including the ATI, HESI and NCLEX.
#NCLEX #ClinicalSkills #HESI #Kaplan #ATI #NursingSchool #NursingStudent #Nurse #RN #PN #Education #LVN #LPN #bedmaking #nurseeducator
00:00 What to expect
00:53 Initial patient position
1:50 Tucking soiled linens
2:20 Placing initial clean linen
3:30 Rolling patient
3:40 Removing soiled linen
4:05 Completing bottom layer
4:33 Changing pillow case
4:50 Top sheet and blanket
7:23 Mitered corner
🚨 Reminder: shipping deadlines are looming 👀
🎁 Regular Shipping: Order by Friday, December 15
🚀 Expedited Shipping: Order by Monday, December 18
🔍 Still searching for last-minute gifts? Consider a Level Up RN Gift Card! 💌 It’s not only a thoughtful present but also the perfect way to share treasures like Pharmacology Flashcards OR digital treasures like Flashables Digital Nursing Flashcards & the Level Up RN membership. Give the gift of knowledge this holiday season! 🧠⚡️💖 bit.ly/LevelUpRNGC
🚪 Access our Cram Courses, Quizzes and Videos all in one ad free space with Level Up RN Membership https://bit.ly/LevelUpRNMembership
Want more ways to MASTER Clinical Skills? Check out our flashcards & videos!
👇👇👇👇👇👇👇👇👇👇
👉 https://bit.ly/clinicalnursingskills 👈
☝️👆☝️👆☝️👆☝️👆☝️👆
This is your one-stop-shop for materials to help you LEARN & REVIEW so you can PASS Nursing School.
🤔🤔🤔 DO YOU WANT TO PASS your classes, proctored exams and the NCLEX? 🤔🤔🤔 Our resources are the best you can buy. They are built with a single goal: help you pass with no fluff. Everything you need, and nothing you don’t. Don’t take our word for it, though! Check out our hundreds of ⭐️⭐️⭐️⭐️⭐️ reviews from nurses who passed their exams and the NCLEX with Level Up RN.
🗂️ Our Ultimate Nursing School Survival kit is your number 1 resource to get through nursing school and to pass the NCLEX. Whether you're just starting school or you’re already prepping for the NCLEX, this bundle of flashcards is the best you can buy. It covers all the information you need to know to pass all your exams and it has FREE shipping!
➡️ https://bit.ly/TUNSSK ⬅️
L👀king for EVEN MORE resources to survive Nursing School? Make your Nursing School experience your own! Life’s difficult enough—learning shouldn’t be.
🪅 Games https://nursesquad.com
💻 Digital resources https://bit.ly/NursingStudyCourses
📅 Organizational tools https://bit.ly/OrganizingSchool
✨Want perks? Join our channel!
https://youtube.com/leveluprn/join
🏷 Head to https://leveluprn.com/specials for all our latest deals!🥳️
📧 LOOKING FOR FREE RESOURCES TO HELP WITH YOUR EXAMS? Get exclusive tips, latest video releases and more delivered to your email!
➡️ https://leveluprn.com/signup ⬅️
⚕ 👩 LEVEL UP NURSE SQUAD 👩⚕️
All of the nurses at Level Up RN are here to help! Cathy Parkes started helping her fellow classmates back when she was in nursing school, tutoring so they could pass their exams and graduate. After she got her BSN and started working as an RN at Scripps Encinitas Hospital, she started this YouTube channel to help nursing students around the world. Since then she has built a team of top-notch dedicated nurses and nurse educators who are focused on improving nursing education and supporting career advancement for nurses everywhere. With flashcards, videos, courses, organizational tools and more, we are singularly focused on helping students and nurses Level Up on their exams and nursing careers.
Learn what's working for other Nursing Students! Check out our Top 10 Most Popular Lessons Here: https://bit.ly/3nda5u3
Get the full lesson here: https://nursing.com/lesson/ski....lls-03-04-trach-care
Welcome to the NURSING Family, we call it the most supportive nursing cohort on the planet.
At NURSING.com, we want to help you remove the stress and overwhelm of nursing school so that you can focus on becoming an amazing nurse.
Check out our freebies and learn more at: (http://www.nursing.com)
Trach Care Overview (Nursing Skills):
In this video we’re going to look at trach care. Remember you should always suction the patient before trach care, so if you haven’t watched that skill video yet, make sure you watch it!
Click here: https://nursing.com/lesson/ski....lls-03-03-trach-suct
And remember as you’re doing this, you want to be assessing the stoma for signs of infection or skin breakdown.
Bookmarks:
0:00 Introduction
0:30 Set up sterile field
1:00 Apply gloves
1:12 Remove inner canula and dressing
1:30 Apply sterile gloves
2:05 Clean secretions
2:56 Clean stoma
3:48 Replace inner canula
4:14 Change trach ties
5:50 Apply dressing
Visit us at https://nursing.com/medical-disclaimer/ for disclaimer information.
NCLEX®, NCLEX-RN® are registered trademarks of the National Council of State Boards of Nursing, INC. and hold no affiliation with NURSING.com.
