- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Alcoholic hepatitis can occur in people who drink heavily for many years. Symptoms include yellow skin and eyes along with increasing belly size due to fluid accumulation. Treatment involves hydration, nutritional care, and stopping alcohol use. Steroid drugs can help reduce liver inflammation.
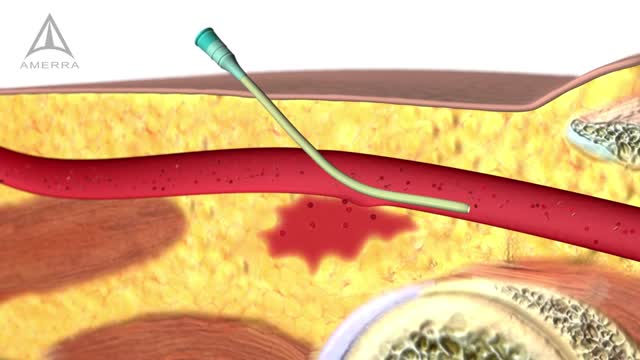
Internal Bleeding Detection
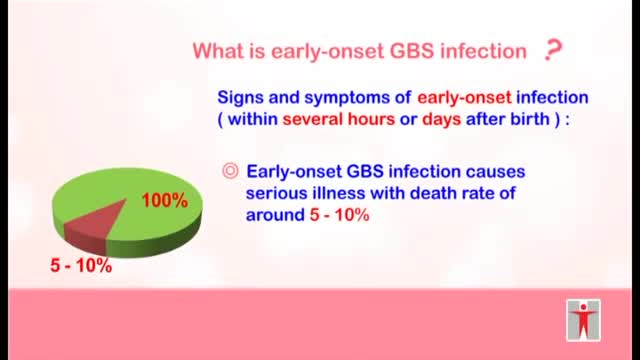
-Intrapartum antibiotic prophylaxis for mothers colonized with group B Streptococcus can prevent early-onset neonatal disease. Adequate prophylaxis consists of ampicillin, penicillin, or cefazolin for ;::4 hours before delivery. Regardless of intrapartum treatment, all high-risk infants must be observed for ;::49 hours. A complete blood count with differential and blood culture are indicated if the infant is preterm <37 weeks or was exposed to prolonged rupture of membranes.>18 hrs.
Cluster headaches, which occur in cyclical patterns or clusters, are one of the most painful types of headache. A cluster headache commonly awakens you in the middle of the night with intense pain in or around one eye on one side of your head. Bouts of frequent attacks, known as cluster periods, can last from weeks to months, usually followed by remission periods when the headaches stop. During remission, no headaches occur for months and sometimes even years. Fortunately, cluster headache is rare and not life-threatening. Treatments can make cluster headache attacks shorter and less severe. In addition, medications can reduce the number of cluster headaches.

Watch that video to see How Snake Poison Coagulates Human Blood
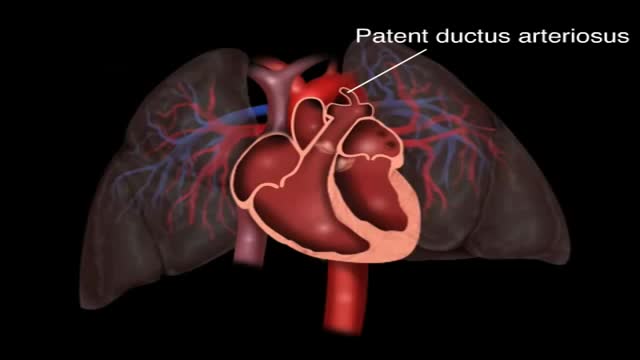
Patent ductus arteriosus (PDA) is a persistent opening between two major blood vessels leading from the heart. The opening, called the ductus arteriosus, is a normal part of a baby's circulatory system before birth that usually closes shortly after birth. If it remains open, however, it's called a patent ductus arteriosus.

Many children receive MRIs at the hospital, and it can often be a scary experience if they are unprepared or don't know what to expect.

A pulmonary embolism (PE) usually happens when a blood clot called a deep vein thrombosis (DVT), often in your leg, travels to your lungs and blocks a blood vessel. That leads to low oxygen levels in your blood. It can damage the lung and other organs and cause heart failure, too. A PE can be life-threatening, so if you've been diagnosed with DVT, you should be aware of this risk. Follow the treatment plan for your DVT to stop the clot from getting bigger and to keep new clots from forming. Symptoms and Diagnosis PE won't always cause symptoms. You might have: Chest pain, which may get worse with a deep breath Sudden shortness of breath or rapid breathing Fast heartbeat Sudden cough Coughing up blood Lightheadedness or fainting Anxiety Call 911 if you notice these symptoms. They could also be symptoms of a heart attack, pneumonia, or other serious problems.

High volume sinus irrigation!
VR medical training takes you inside the human body.
Today, hair transplant physicians are able to make use of different techniques to extract and transplant large numbers of hair follicles (follicular units). There are two primary techniques for hair transplantation currently in use. The FUE (Follicular Unit Extraction) and the FUT (Follicular Unit Transplantation) methods. They differ primarily in the way hair follicles are extracted from the donor area. Follicular Unit Transplantation (FUT) The FUT process involves removing a small strip of tissue from the back of the head, from which the donor hair follicles will be extracted. The hair follicles are harvested from the strip by a skilled clinical team before being individually transplanted to the recipient areas. In most cases, and especially cases of advanced hair loss, FUT is the preferred method because it allows the physician to fully utilize the scalp area to deliver results consistent with patient expectations. FUT typically allows for the greatest number of grafts to be transplanted in a single session. Pain Management Some patients report higher levels of discomfort with FUT procedures compared to FUE due the potential swelling in the area where the strip of tissue was removed, but both methods have a very manageable recovery period and pain medication can be prescribed by your physician if needed. Both techniques of hair transplantation are relatively simple. Hair transplantation procedures are outpatient surgeries with some patients going back to work as soon as the very next day. Scarring The FUT strip extraction method typically results in a very narrow linear scar in the back of the head (typically 1mm in diameter or less in size). Since the scar is very thin, it’s easily concealed by all but the shortest of haircut styles. A short to moderate crop setting on most clippers is sufficient to conceal the scar for the majority of patients, and over time the scar will become less noticeable as it fades. Costs The industry norm for pricing is on a per-graft basis. This allows each individual to pay for only what they need and receive in number of grafts, and not a flat rate that in the end may cost you more. The per-graft cost of a FUT procedure is generally lower than that of a FUE procedure. Lately however, in response to the rising popularity of the FUE technique, many hair transplantation clinics have started lowering the per graft cost on FUE procedures, so that the cost difference between the two types of procedure are not as much as most people think. The costs of medical procedures always vary by patients’ conditions, needs and objectives. For the most accurate assessment of your hair loss and the associated cost of your hair restoration, you will need to speak to a physician. Follicular Unit Extraction (FUE) In an FUE hair transplantation, each follicular unit is individually taken directly from the scalp with no strip of tissue being removed. Hair follicles are removed in a random fashion and the result is less density in the donor area that many say is not even noticeable. This is the main difference between FUE & FUT. Since follicles are removed one at a time, fewer follicles can be harvested during a typical session, making FUE a better option to restore hair in smaller cases (number of grafts) compared to the traditional FUT method. FUE is constantly evolving and what was once utilized for only smaller cases is now being utilized for larger and larger cases. Some people that prefer the FUE method may have the option of splitting their procedure into two days in order to complete their recommended transplantation goals. Pain Management With no stitches required and no linear scar left to heal, FUE procedures do have a faster healing time and less post-procedure discomfort compared to the traditional FUT procedure. Scarring Since FUE procedures involve removing hairs individually from the scalp, there is no linear scar left behind. However, there will be tiny 1mm in diameter or less puncture marks that tend to heal by themselves after scabbing-over in the days following the procedure. These tiny wounds typically heal within three to seven days. Costs Since the physician must remove each hair follicle individually, the time-sensitive nature of an FUE procedure typically makes it more expensive than an FUT procedure. As stated earlier, FUE technology is improving as well as gaining popularity and many hair restoration practices (including Bosley) have started to lower the cost per graft price for FUE procedures. Nowadays, the cost difference between a FUE and a FUT procedures is less disparate.

Labiaplasty is a surgical procedure that removes excess tissue from the labia, either for cosmetic reasons or for women who feel physical discomfort due to enlarged or elongated labia

Soft tissue biopsy from osteolytic lesions is a challenge for the interventionist. The Spirotome Bone is conceived for this intervention. The procedure is straigthforward and produces tissue specimens of high quality in sufficient amounts to allow quantitative molecular biology.

Gowers' sign is a medical sign that indicates weakness of the proximal muscles, namely those of the lower limb. The sign describes a patient that has to use his hands and arms to "walk" up his own body from a squatting position due to lack of hip and thigh muscle strength. It is named for William Richard Gowers. Gowers' sign is classically seen in Duchenne muscular dystrophy, but also presents itself in centronuclear myopathy, myotonic dystrophy and various other conditions associated with proximal muscle weakness. For this maneuver, the patient is placed on the floor away from any objects that could otherwise be used to pull oneself to a standing position. It is also used in testing paraplegia.

The 30 minute DVD:
introduces moving and handling of people
describes safer people handling practices
features specialist guidance from a chartered physiotherapist
outlines the process for people handling risk assessments
sets out the principles of safer handling
demonstrates the key safer handling techniques:
rolling a person
inserting and removing sliding sheets
repositioning people using sliding sheets
assisting people to stand and walk with handling belts
the use of roll boards in lateral transfers
using hoists
highlights the important role you play in safer people handling
M. D. Anderson Cancer Center provides a basic education on cancer.
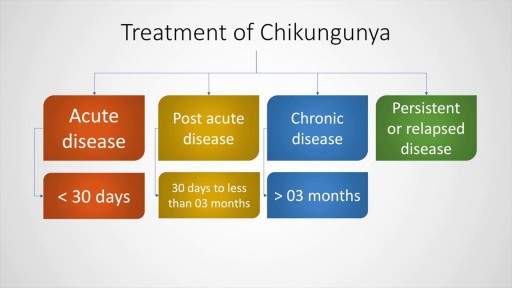
A decade ago we thought that Chikungunya was a tropical disease restricted to the rain forests. However, after the 2007 epidemic in Italy and later in the Reunion islands, this dreaded condition has now spread to the Carribean and the Americas. Its an arthropod borne alpha virus which causes fever, polyarthralgia and arthritis. There could be serious complications in the adult such as meningoencephalitis or GBS as well as in neonates. This presentation discusses in detail the clinical features, diagnosis and management of Chikungunya fever. A detailed discussion of its complications is also included. Check out our other videos

Frostbite is an injury caused by freezing of the skin and underlying tissues. First your skin becomes very cold and red, then numb, hard and pale. Frostbite is most common on the fingers, toes, nose, ears, cheeks and chin. Exposed skin in cold, windy weather is most vulnerable to frostbite. But frostbite can occur on skin covered by gloves or other clothing.

Uterine rupture is usually when the scar from your previous caesarean section tears open. Though it's uncommon, you should be aware of this risk, particularly if you're thinking about giving birth vaginally next time. It's possible for your scar to gape slightly while you're pregnant (scar dehiscence).

Common causes of the knee pain
Knee pain is very common and in this video we will present the most common problems that can cause pain in the knee. (Patella) itself, which is in front of the knee, or from the tendons that are attached to the kneecap (patellar tendon and quadricep tendon). One of the most common problems is patellar chondromalacia which is chronic pain due to the softening of the cartilage beneath the kneecap. The cartilage of the kneecap will have some erosions, defects, or holes from mild to complete inside the joint (exactly in the back of the kneecap).
• Pain in the front of the knee
• Occurs more in young people
• Becomes worse from climbing up stairs and going downstairs
Treatment is usually nonsteroidal anti-inflammatory medication, physical therapy, and surgery is very rare. Also in front of the kneecap, the patient may get pain due to prepatellar bursitis.
When there is prepatellar bursitis, the patient will see that the swelling, the inflammation, and the pain is located over the front of the kneecap. The bursa becomes inflamed and fills with fluid at the top of the knee, causing pain, swelling, tenderness and a lump in that area on top of the kneecap. If the pain is in front of the knee but below or above the patella, this may indicate that the patient has tendonitis. Patellar tendonitis is an overuse condition that often occurs in athletes who perform repetitive jumping activities. Patellar tendonitis is a knee pain that is associated with focal patellar tendon tenderness and it is usually activity related. It is located below the kneecap and is called "jumper's knee". Patellar tendonitis affects approximately 20% of jumping athletes. There will be tenderness to palpation at the distal pole of the patella in extension and not in flexion. Quadriceps inflexibility, atrophy and hamstring tightness are predisposing factors for this condition. Treatment is rest, anti-inflammatory medication, stretching and strengthening of the hamstrings and quadriceps. Use an eccentric exercise program. The early stages of patellar tendonitis will respond well to nonoperative treatment. Another important cause of knee pain is a meniscal tear. The meniscus is the cushion that protects the cartilage in the knee. Injury will cause pain on the medial or the lateral side of the knee exactly at the level of the joint. The patient will complain of a history of locking, instability and swelling of the knee. McMurray test will be positive. A painful pop or click is obtained as the knee is brought from flexion to extension with either internal or external rotation of the knee. Arthritis of the knee Knee arthritis is very common. The cartilage cells die with age and its repair response decreases in the joint collapses with increased breakdown of the framework of the cartilage. The patient will have progressive blurring away of the cartilage of the joint with decreased joint space as seen on x-rays. Another source of pain is the Baker's cyst. The cyst is in the back of the knee between the semimembranosus yes and the medial gastrocnemius muscles. Another important source of knee pain is a ligament injury. Here is a normal knee without a ligament injury. Here you can see from the front, you can see the lateral and medial collateral ligament. You can see the ACL and PCL from the side view. These ligaments are usually injured as a result of a sports activity. Here is an example of a sports knee injury. Here is an example of the medial collateral ligament injury. This is the most commonly injury knee ligament injury to this ligament is on the inner part of the knee. Here is an example of an injury of the anterior cruciate ligament. It involves a valgus stress to the knee. Lachman test is usually positive, and MRI is diagnostic. Another important cause of knee pain is iliotibial band syndrome of the knee. Inflammation of the thickening of the iliotibial band results from excessive friction as the iliotibial band slides over the lateral femoral condyle. The iliotibial band is a thick band of fascia that extends along the lateral thigh from the iliac crest to the knee. And as the knee moves, the IT band was repeatedly shifted forwards and backwards across the lateral femoral condyle. The patient will complain of swelling, tenderness, and crepitus over the lateral femoral condyle. The condition occurs in the ITB S occurs in runners, cyclist and athletes that require repeated knee flexion and extension. The pain may be reproduced by doing a single-leg squat. The Ober's test is used to at assess tightness of the iliotibial band. MRI may show edema in the area of the ITB. Treatment is usually nonoperative with rest and ice, physical therapy, with stretching, proprioception, and improvement in neuromuscular coordination. Training modification and injections may be helpful. Surgery is a last resort. Surgical excision of the scarred inflamed part of the iliotibial band.
