סרטונים מובילים

Incision and Drainage of a Huge Gluteal Abscess

Delivery using foreceps

This video demonstrates the use of an episiotomy to facilitate vaginal delivery of a baby

The products of a surgical abortion.
Lack of sunshine causes skin cancer, according to Andreas Moritz. In this video from 2009, he explains why being in the sun is actually good for you and your skin. Find out why your sunscreen is doing more harm than good. Also, you need vitamin D to prevent cancer, and sunscreen may interfere with your exposure to vitamin D from the sun.

Types of breast cancer. The different types of breast cancer carry with them different prognosis and different treatment options
This video gives you an overview of how a cardiac catheterization is performed.
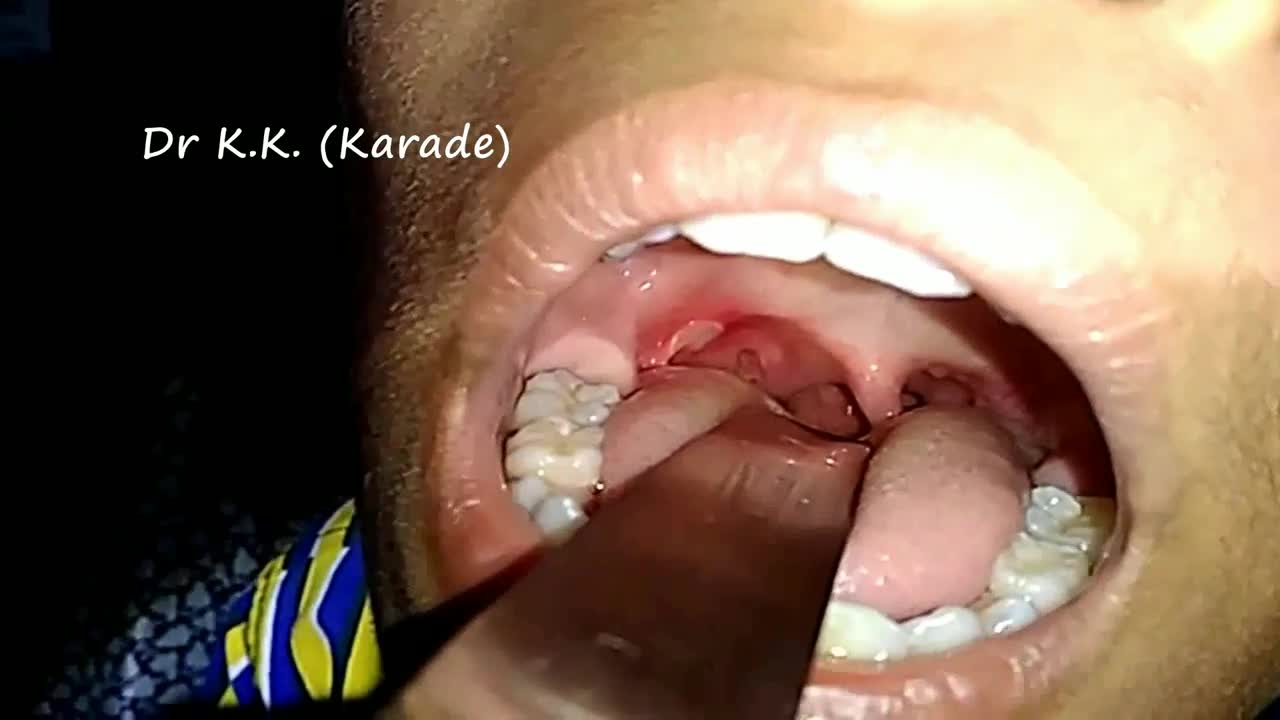
Canker sores (Aphthous ulcer) are small, painful ulcers on the inside of the mouth, tongue, lips, or throat.Canker sores are white or yellow and surrounded by a bright red area. They are not cancerous.
Extradural approach via Orbito-Zygomatic Craniotomy

This is a video of a Gender Reassignment Surgery, watch as surgeons change a male to a female its an extremely interesting procedure

"The act of cutting off the prepuce or foreskin of males, or the internal labia of females." Webster's Revised Unabridged Dictionary (1913)

Nosebleeds are common due to the location of the nose on the face, and the large amount of blood vessels in the nose. The most common causes of nosebleeds are drying of the nasal membranes and nose picking (digital trauma), which can be prevented with proper lubrication of the nasal passages and not picking the nose.
http://www.wss4m.com/vb
The 3rd Annual W. B. Ingalls Memorial
Prostate Health and Cancer Seminar features nationally renowned physicians and scientists presenting the most current study and practices for the diagnosis and treatment of prostate cancer. This day-long program offers in-depth exploration of prostate issues that range from monitoring PSA counts to cutting-edge research to current treatment trends.

NOVEL METHOD: REAL ANATOMIC CUSTOM-MADE IMMEDIATE ZIRCONIA IMPLANT. YOUR DENTAL ROOT IS MILLED IN ZIRCONIA AND IN JUST 2 MINUTES SEATED, NO DRILLING, NO AUGMENTATION, NO MEMBRANES, FLAPLESS, NO 3D PLANNING, NO CAD/CAM SPLINTS OR GUIDED SURGERY REQUIRED! EASY AND CONSEQUENTIAL SYSTEM. NO MORE INCONGRUOUS AND UGLY SILVER-COLORED TITANIUM IMPLANTS IN TIME CONSUMING, PAINFUL AND COSTLY PROCEDURES. IT`S HIGH TIME TO RESPECT THE ANATOMY NOT ALTER IT BY DRILLING AND AUGMENTATION. BIOIMPLANT

Frostbite is an injury caused by freezing of the skin and underlying tissues. First your skin becomes very cold and red, then numb, hard and pale. Frostbite is most common on the fingers, toes, nose, ears, cheeks and chin. Exposed skin in cold, windy weather is most vulnerable to frostbite. But frostbite can occur on skin covered by gloves or other clothing. Frostnip, the first stage of frostbite, doesn't cause permanent skin damage. You can treat very mild frostbite with first-aid measures, including rewarming your skin. All other frostbite requires medical attention because it can damage skin, tissues, muscle and bones. Possible complications of severe frostbite include infection and nerve damage.
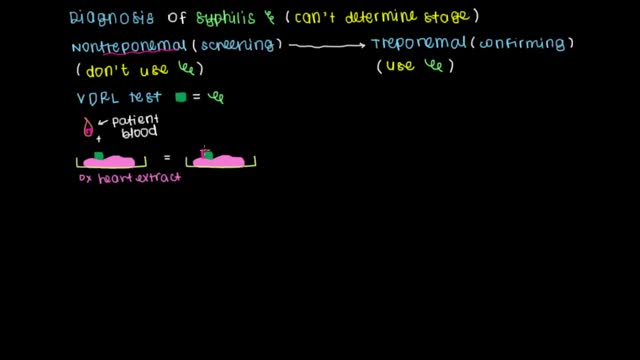
Learn what tests can be used to screen and diagnose syphilis as well as how to treat and prevent the infection.

A video showing the process of childbirth via vaginal delivery.

Mammogram are great technologies, however, sometimes it cannot detect many things under our bodies. In this video, Dr. Linder is performing a breast implant removal and revision on a patient who has a rupture breast implants. Dr. Stuart Linder is a Beverly Hills board certified plastic surgeon, specializing in body sculpting and reconstructive procedures including breast augmentation, reduction, lift, liposuction and tummy tuck. He is board-certified by the American Board of Plastic Surgery and is affiliated with the American College of Surgeons, the American Society of Plastic and Reconstructive Surgeons and the American Medical Association.

Watch How Snake Poison Could Turn Human Blood Into Jelly
