Los mejores videos

Ingrown Hair Removal Video


watch that video of Popping a Huge Hand Burn Blister

Longest Ingrown Hair Removal

Ascites, the collection of fluid within the peritoneal space is caused due to a variety of causes including cirrhosis, cardiac causes, sinusoidal obstruction syndrome, tubercular peritonitis and pancreatitis, amongst others. Most commonly, the cause of ascots may be cirrhosis , which in turn, is most frequently causes by alcohol use, hepatitis C and non-alcoholic steatohepatitis. At the heart of the ascitic fluid analysis is the serum albumin ascitic gradient, the differential diagnosis of which has been discussed in detail in this presentation. Both low SAAG and high SAAG ascites have been dealt with in some depth, with a brief overview of the management of these conditions

Watch that video of an Ingrown hair turned into 140-pound tumor in man’s stomach
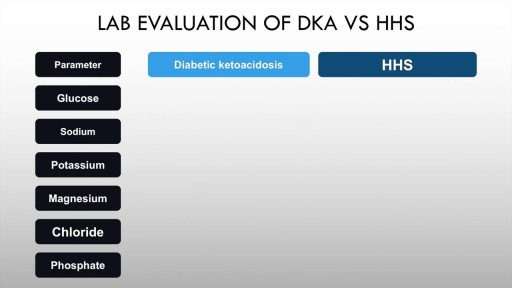
Diabetic ketoacidosis is an acute complication of uncontrolled hyperglycaemia characterised by high anion gap metabolic acidosis, dehydration and other metabolic abnormalities. Upto half of patients with Type 1 diabetes mellitus may have DKA. The incidence in T2DM is also rising. Precipitants include acute illness such as myocardial infarction, trauma and infection. Paitents of diabetic ketoacidosis may present with vomiting, pain abdomen and lethargy. Mental obtundation may also be present. Management of diabetic ketoacidosis revolves around administration of IV normal saline, insulin, replacement of potassium with frequent monitoring of sugars and electrolytes.

very day, specialists deliver high-quality care in 68 disciplines in health centres across Canada. Yet many Canadians know very little about what many specialists actually do, and the important role these disciplines play in Canada’s health care system. This video provides a brief high-level overview of what Internal Medicine Specialists actually do, their training, and their role in Canadian health care.

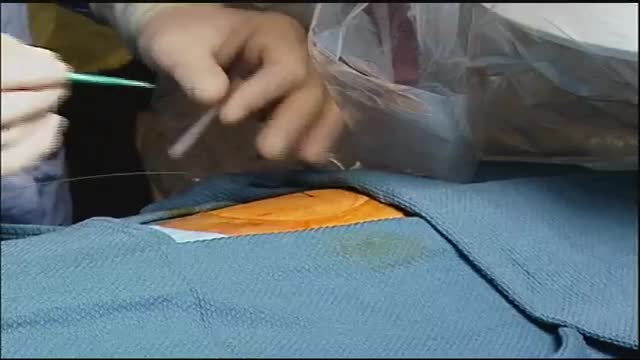
Suprapubic Catheterization / Cystostomy
Idiopathic pulmonary fibrosis (IPF) is defined as a specific form of chronic, progressive fibrosing interstitial pneumonia of unknown cause, primarily occurring in older adults, limited to the lungs, and associated with the histopathologic and/or radiologic pattern of usual interstitial pneumonia (UIP).[1] Signs and symptoms The clinical symptoms of idiopathic pulmonary fibrosis are nonspecific and can be shared with many pulmonary and cardiac diseases. Most patients present with a gradual onset (often >6 mo) of exertional dyspnea and/or a nonproductive cough. Approximately 5% of patients have no presenting symptoms when idiopathic pulmonary fibrosis is serendipitously diagnosed.

Use warm water and sea salt. Soak the wart for 10 to 15 minutes in warm salt water to moisten the skin. Scrape the dead skin layers off the wart using a nail file, pumice stone or mild sandpaper. You could also use your fingers, but wash them thoroughly before and after, as warts can easily spread.

A torn meniscus is one of the most common knee injuries. Any activity that causes you to forcefully twist or rotate your knee, especially when putting your full weight on it, can lead to a torn meniscus. Each of your knees has two menisci — C-shaped pieces of cartilage that act like a cushion between your shinbone and your thighbone. A torn meniscus causes pain, swelling and stiffness. You also might feel a block to knee motion and have trouble extending your knee fully. Conservative treatment — such as rest, ice and medication — is sometimes enough to relieve the pain of a torn meniscus and give the injury time to heal on its own. In other cases, however, a torn meniscus requires surgical repair.
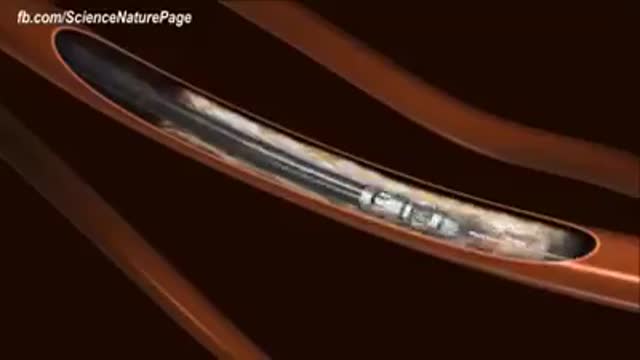
An intra-aortic balloon pump (IABP) is a mechanical device that helps the heart pump blood. This device is inserted into the aorta, the body's largest artery. It is a long, thin tube called a catheter with a balloon on the end of it. If you are hospitalized, your doctor may insert an IABP.
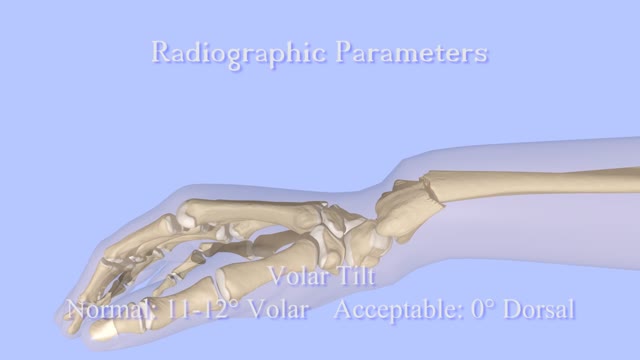
Closed Reduction of Distal Radius Fractures - Discussion: (distal radius fracture menu) - closed reduction & immobilization in plaster cast remains accepted method of treatment for majority of stable distal radius frx; - unstable fractures will often lose reduction in the cast and will slip back to the pre-reduction position; - patients should be examined for carpal tunnel symptoms before and after reduction; - carpal tunnel symptoms that do not resolve following reduction will require carpal tunnel release; - cautions: - The efficacy of closed reduction in displaced distal radius fractures. - Technique: - anesthesia: (see: anesthesia menu) - hematoma block w/ lidocaine; - w/ hematoma block surgeon should look for "flash back" of blood from hematoma, prior to injection; - references: - Regional anesthesia preferable for Colles' fracture. Controlled comparison with local anesthesia. - Neurological complications of dynamic reduction of Colles' fractures without anesthesia compared with traditional manipulation after local infiltration anesthesia. - methods of reduction: - Jones method: involves increasing deformity, applying traction, and immobilizing hand & wrist in reduced position; - placing hand & wrist in too much flexion (Cotton-Loder position) leads to median nerve compression & stiff fingers; - Bohler advocated longitudinal traction followed by extension and realignment; - consider hyper-extending the distal fragment, and then translating it distally (while in extended position) until it can be "hooked over" proximal fragment; - subsequently, the distal fragment can be flexed (or hinged) over the proximal shaft fragment; - closed reduction of distal radius fractures is facilitated by having an assistant provide counter traction (above the elbow) while the surgeon controls the distal fragment w/ both hands (both thumbs over the dorsal surface of the distal fragment); - flouroscopy: - it allows a quick, gentle, and complete reduction; - prepare are by prewrapping the arm w/ sheet cotton and have the plaster or fibroglass ready; - if flouroscopy is not available, then do not pre-wrap the extremity w/ cotton; - it will be necessary to palpate the landmarks (outer shaped of radius, radial styloid, and Lister's tubercle, in order to judge success of reduction; - casting: - generally, the surgeon will use a pre-measured double sugar sugar tong splint, which is 6-8 layers in thickness; - more than 8 layers of plaster can cause full thickness burns: - reference: Setting temperatures of synthetic casts. - position of immobilization - follow up: - radiographs: - repeat radiographs are required weekly for 2-3 weeks to ensure that there is maintenance of the reduction; - a fracture reduction that slips should be considered to be unstable and probably require fixation with (pins, or ex fix ect.) - there is some evidence that remanipulation following fracture displacement in cast is not effective for these fractures; - ultimately, whether or not a patient is satisfied with the results of non operative treatment depends heavily on th
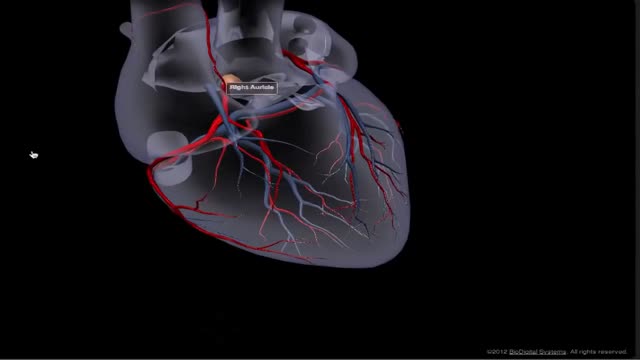
The heart receives its own supply of blood from the coronary arteries. Two major coronary arteries branch off from the aorta near the point where the aorta and the left ventricle meet. These arteries and their branches supply all parts of the heart muscle with blood.
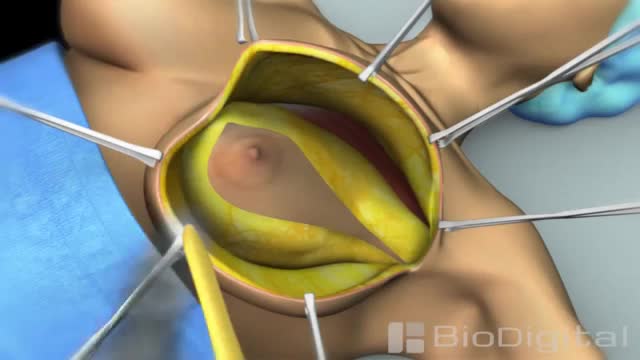
Mastectomy is surgery to remove all breast tissue from a breast as a way to treat or prevent breast cancer. For those with early-stage breast cancer, mastectomy may be one treatment option. Breast-conserving surgery (lumpectomy), in which only the tumor is removed from the breast, may be another option.
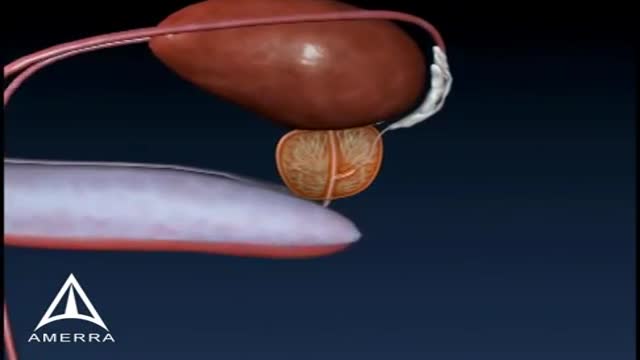
Prostate biopsy is a procedure in which small hollow needle-core samples are removed from a man's prostate gland to be examined microscopically for the presence of cancer. It is typically performed when the result from a PSA blood test rises to a level that is associated with the possible presence of prostate cancer.
Radiosurgery: Radiosurgery devices, such as the CyberKnife Robotic Radiosurgery System, offer patients a new option for the treatment of lung cancer. The CyberKnife® System is used to treat lung cancer patients who cannot tolerate surgery, have an inoperable tumor, or are seeking an alternative to surgery.
Cholesterol is a fat-like, waxy substance that can be found in all parts of your body. It helps your body make cell membranes, many hormones, and vitamin D. The cholesterol in your blood comes from two sources: the foods you eat and your liver. But your liver makes all the cholesterol your body needs.

A new and safer method of inserting a Foley catheter suprapubically. The technique allows the insertion to be carried out in an Outpatient setting, thus saving time, cost and effort. By using the Seldinger technique, the product reduces the chances of bowel or bladder perforation and resultant morbidity.
The product has been chosen by The NHS National Technology Adoption Centre to help facilitate adoption of the product.
See www.mediplus.co.uk for more information
