- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Adult stem cells are cells from your own body that can renew themselves and turn into other cells (differentiate). They live inside all of us in various tissues, poised to leap into action to repair damage as it occurs. As we age or have big injuries, we may not be able to recruit enough of these cells to the site to fully repair the area. Regenexx Stem Cell Procedures help overcome this problem by extracting stem cells from an area of high volume, then concentrating the cells and reinjecting them into the damaged area to help the body heal naturally.

Paracentesis is a procedure to take out fluid that has collected in the belly (peritoneal fluid). This fluid buildup is called ascites camera.gif. Ascites may be caused by infection, inflammation, an injury, or other conditions, such as cirrhosis or cancer. The fluid is taken out using a long, thin needle put through the belly. The fluid is sent to a lab and studied to find the cause of the fluid buildup. Paracentesis also may be done to take the fluid out to relieve belly pressure or pain in people with cancer or cirrhosis.
Ovarian dermoid cyst and mature cystic ovarian teratoma are terms often used interchangeably to refer to the most common ovarian neoplasm. These slow-growing tumours contain elements from multiple germ cell layers and are best assessed with ultrasound.
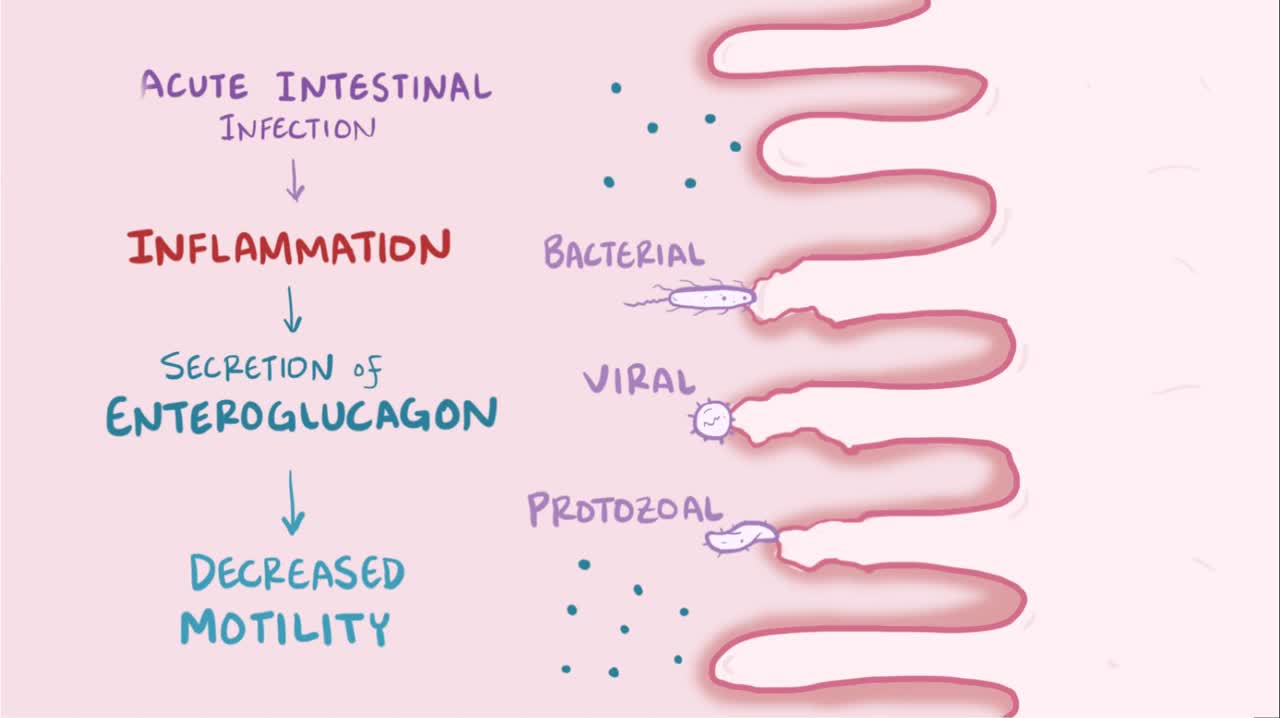
What is tropical sprue? Tropical sprue is diagnosed when somebody has long-standing GI problems and has visited tropical regions in the past. It's thought to be caused by bacterial overgrowth and often leads to villous atrophy.
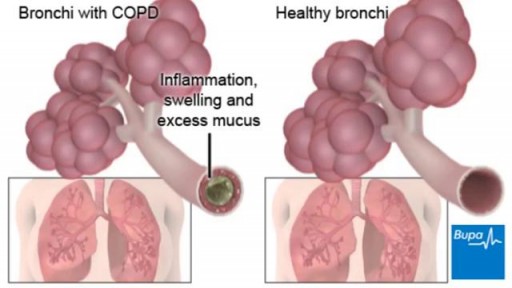
COPD (chronic obstructive pulmonary disease) makes it hard for you to breathe. The two main types are chronic bronchitis and emphysema. The main cause of COPD is long-term exposure to substances that irritate and damage the lungs. This is usually cigarette smoke. Air pollution, chemical fumes, or dust can also cause it. At first, COPD may cause no symptoms or only mild symptoms. As the disease gets worse, symptoms usually become more severe. They include A cough that produces a lot of mucus Shortness of breath, especially with physical activity Wheezing Chest tightness Doctors use lung function tests, imaging tests, and blood tests to diagnose COPD. There is no cure. Treatments may relieve symptoms. They include medicines, oxygen therapy, surgery, or a lung transplant. Quitting smoking is the most important step you can take to treat COPD.
Watch that video to know if oral sex can cause cancer

The Epley maneuver is a series of movements, normally carried out on a person by a doctor, to relieve the symptoms of BPPV. Research has found it to be an easy, safe, and effective treatment for the condition in both the long- and short-term. The Epley maneuver is sometimes called the particle repositioning maneuver or the canalith repositioning maneuver. These names are used because the maneuver involves a series of movements that help to reposition crystals in a person's ear that may cause feelings of dizziness. Repositioning the crystals helps to relieve the person's dizziness and nausea.

If you go to research LASIK eye surgery online, you may get conflicting messages. Some articles rave about it, but in some cases, others link it to severe pain or even suicide. 7 Action News' Carolyn Clifford sat down with one of the area's biggest providers of eye surgery to try and separate fact from fiction, so if you go under the laser, you know the risk.
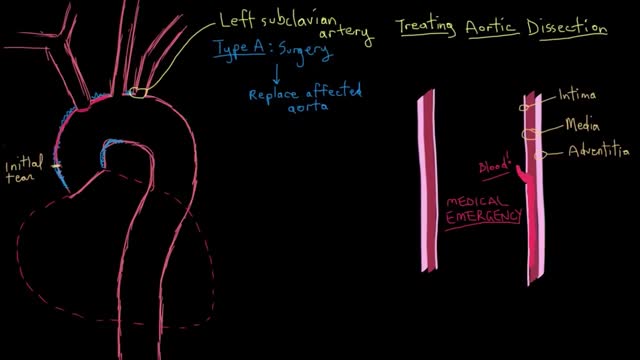
Acute aortic dissection can be treated surgically or medically. In surgical treatment, the area of the aorta with the intimal tear is usually resected and replaced with a Dacron graft. Emergency surgical correction is the preferred treatment for Stanford type A (DeBakey type I and II) ascending aortic dissection. It is also preferred for complicated Stanford type B (DeBakey type III) aortic dissections with clinical or radiologic evidence of the following conditions: Propagation (increasing aortic diameter) Increasing size of hematoma Compromise of major branches of the aorta Impending rupture Persistent pain despite adequate pain management Bleeding into the pleural cavity Development of saccular aneurysm

Pregnancy is one of the beautiful phases of a woman’s life after their marriage. The feeling of the baby growing inside the womb is exceptional and very special.
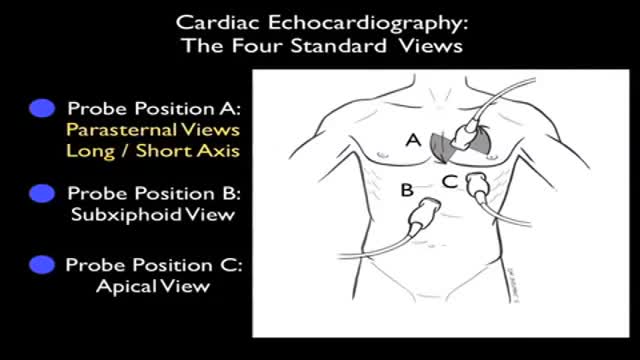
Ultrasound of Heart

I filmed my lasik eye surgery because it looks neat
See the full video here: https://youtu.be/wY_D5pMbEf0
Subscribe to my main channel: https://www.youtube.com/channe....l/UC1VLQPn9cYSqx8plb
#shorts
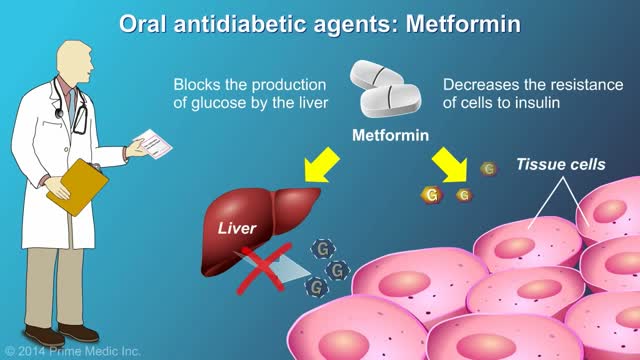
protecting the body from damage caused by hyperglycemia cannot be overstated. In the United States, 57.9% of diabetic patients have one or more diabetes complications, and 14.3% have three or more.1 Strict glycemic control is the primary method of reducing the development and progression of microvascular complications, such as retinopathy, nephropathy, and neuropathy. Aggressive treatment of dyslipidemia and hypertension decreases macrovascular complications.2-4 Glycemic Control There are two primary techniques available for physicians to assess the quality of a patient’s glycemic control: self-monitoring of blood glucose (SMBG) and interval measurement of hemoglobin A1c (HbA1c).
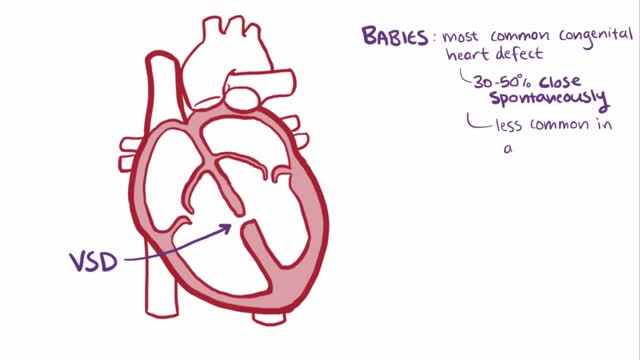
A ventricular septal defect (VSD), a hole in the heart, is a common heart defect that's present at birth (congenital). The hole occurs in the wall that separates the heart's lower chambers (septum) and allows blood to pass from the left to the right side of the heart. The oxygen-rich blood then gets pumped back to the lungs instead of out to the body, causing the heart to work harder. A small ventricular septal defect may cause no problems, and many small VSDs close on their own. Larger VSDs need surgical repair early in life to prevent complications.
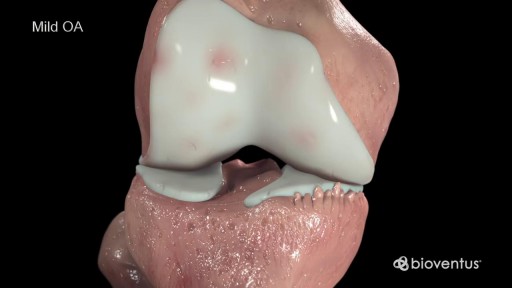
Cartilage is a slippery tissue that provides a smooth surface for joint motion and acts as a cushion between the bones. Synovium is soft, and it lines the joints. It produces fluid, called synovial fluid, for lubrication, and it supplies nutrients and oxygen to the cartilage. As these functions break down, they no longer protect the bones of the knee joint, and bone damage occurs. OA of the knee can cause pain and stiffness. The symptoms worsen over time
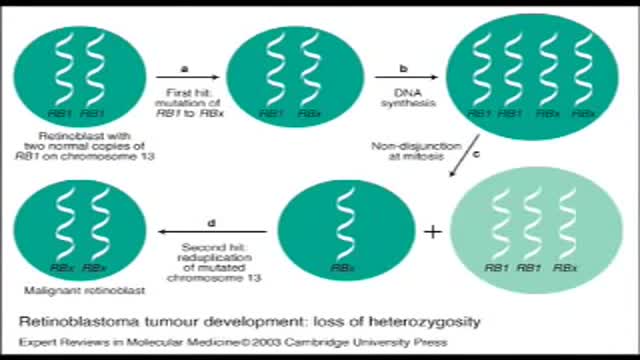
Retinoblastoma is an eye cancer that begins in the retina — the sensitive lining on the inside of your eye. Retinoblastoma most commonly affects young children, but can rarely occur in adults. Your retina is made up of nerve tissue that senses light as it comes through the front of your eye. The retina sends signals through your optic nerve to your brain, where these signals are interpreted as images. A rare form of eye cancer, retinoblastoma is the most common form of cancer affecting the eye in children. Retinoblastoma may occur in one or both eyes.

Carpal tunnel syndrome is a hand condition that causes numbness, tingling and other symptoms. Carpal tunnel syndrome is caused by a pinched nerve in your wrists A number of factors can contribute to carpal tunnel syndrome, including the anatomy of your wrist, certain underlying health problems and possibly patterns of hand use. Bound by bones and ligaments, the carpal tunnel is a narrow passageway located on the palm side of your wrist. This tunnel protects a main nerve to your hand and the nine tendons that bend your fingers. Compression of the nerve produces the numbness, tingling and, eventually, hand weakness that characterize carpal tunnel syndrome.

Anemia is a medical condition in which the red blood cell count or hemoglobin is less than normal. The normal level of hemoglobin is generally different in males and females. For men, a normal hemoglobin level is typically defined as a level of more than 13.5 gram/100 ml, and in women as hemoglobin of more than 12.0 gram/100 ml. These definitions may vary slightly depending on the source and the laboratory reference used. Continue Reading

Watch that video of Female Genital Infection Causes and Symptoms
Aortic valve replacement is a procedure in which a patient's failing aortic valve is replaced with an artificial heart valve. The aortic valve can be affected by a range of diseases; the valve can either become leaky (aortic insufficiency / regurgitation) or partially blocked (aortic stenosis).
