शीर्ष वीडियो
Learn about Bicuspid Aortic Valves in this presentation. Bicuspid Aortic Valves are present in about 2% of the population and are the most common congenital disorder. Find out more about a Bicuspid Aortic Valve by visiting the following link:
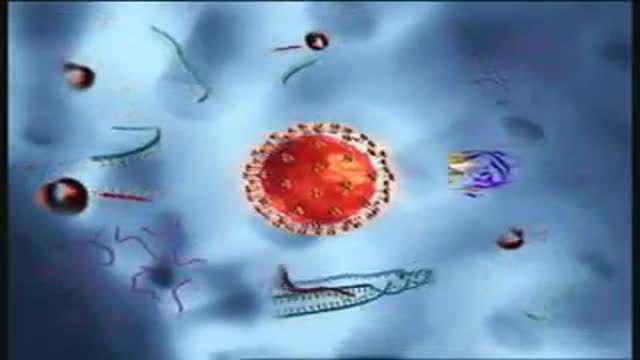
Binding and Fusion: HIV begins its life cycle
when it binds to a CD4 receptor and one of two
co-receptors on the surface of a CD4+
Tlymphocyte. The virus then fuses with the host
cell. After fusion, the virus releases RNA, its
genetic material, into the host cell.
Reverse Transcription: An HIV enzyme
called reverse transcriptase converts the singlestranded HIV RNA to double-stranded HIV DNA.
Integration: The newly formed HIV DNA
enters the host cell's nucleus, where an HIV
enzyme called integrase "hides" the HIV DNA
within the host cell's own DNA. The integrated
HIV DNA is called provirus. The provirus may
remain inactive for several years, producing few or
no new copies of HIV
Transcription: When the host cell receives a
signal to become active, the provirus uses a host
enzyme called RNA polymerase to create copies of
the HIV genomic material, as well as shorter
strands of RNA called messenger RNA (mRNA).
The mRNA is used as a blueprint to make long
chains of HIV proteins.
Assembly: An HIV enzyme called protease cuts
the long chains of HIV proteins into smaller
individual proteins. As the smaller HIV proteins
come together with copies of HIV's RNA genetic
material, a new virus particle is assembled.
Budding: The newly assembled virus pushes out
("buds") from the host cell. During budding, the new
virus steals part of the cell's outer envelope. This
envelope, which acts as a covering, is studded with
protein/sugar combinations called HIV
glycoproteins. These HIV glycoproteins are
necessary for the virus to bind CD4 and coreceptors. The new copies of HIV can now move
on to infect other cells.

Learn more about certified electronic health record and comprehensive hospital information system (HIS), Paragon®, from McKesson. Working with Paragon can help you achieve Stage 1 meaningful use and other important guidelines.

laparoscopic appendcectomy
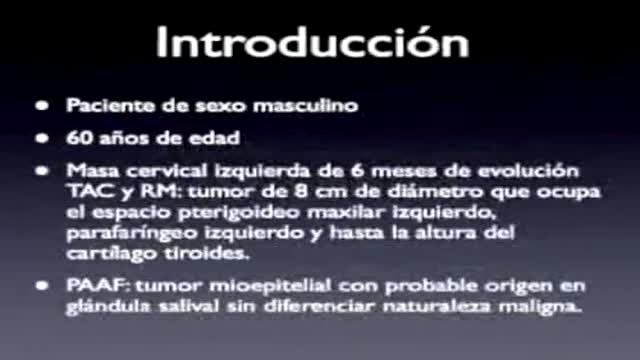
PARAPHARYNGEAL SPACE TUMORS: SURGICAL APPROACH

Dr. Ed Tingstad, Orthopedic Surgeon with Pullman Regional Hospital’s Orthopedic Center of Excellence and Inland Orthopaedic Surgery & Sports Medicine Clinic performs a total knee replacement using orthopedic robotics – VELYS. The VELYS Robotic-Assisted Solution technology makes for a more exact fitting knee replacement and uses intra-operative data to inform the surgeon during surgery. In this full-length total knee replacement video, Dr. Tingstad narrates a procedure from start to finish.
Learn more: pullmanregional.org/orthopedics

Watch that Complete Chopped Hand Microvascular Re-implantation Surgery

Soon enough, a robot will be doing surgeries on you!

MASSIVE Goose Egg Drained

Watch that video of Removing Hundreds of Worms Living Inside Teeth


A pelvic mass is a general term for any growth or tumor on the ovary or in the pelvis. A pelvic mass can be cystic (cystadenoma), solid (fibroma), or both (dermoid). A pelvic mass can be benign or malignant.
Electrical injuries can present with a variety of problems, including cardiac or respiratory arrest, coma, blunt trauma, and severe burns of several types. It is important to establish the type of exposure (high or low voltage), duration of contact, and concurrent trauma. Low-voltage AC injury without loss of consciousness and/or arrest These injuries are exposures of less than 1000V and usually occur in the home or office setting. Typically, children with electrical injuries present after biting or chewing on an electrical cord and suffer oral burns. Adults working on home appliances or electrical circuits can also experience these electrical injuries. Low-voltage AC may result in significant injury if there is prolonged, tetanic muscle contraction. Low-voltage AC injury with loss of consciousness and/or arrest In respiratory arrest or ventricular fibrillation that is not witnessed, an electrical exposure may be difficult to diagnose. All unwitnessed arrests should include this possibility in the differential diagnosis. Query EMS personnel, family, and coworkers about this possibility. Inquire if a scream was heard before the patient’s collapse; this may be due to involuntary contraction of chest wall muscles from electrical current. High-voltage AC injury without loss of consciousness and/or arrest Usually high-voltage injuries do not cause loss of consciousness but instead cause devastating thermal burns. In occupational exposures, details of voltage can be obtained from the local power company. High-voltage AC injury with loss of consciousness and/or arrest This is an unusual presentation of high-voltage AC injuries, which do not often cause loss of consciousness. History may need to come from bystanders or EMS personnel. Direct current (DC) injury These injuries typically cause a single muscle contraction that throws the victim away from the source. They are rarely associated with loss of consciousness unless there is severe head trauma, and victims can often provide their own history. Conducted electrical devices Conducted electrical weapons (CEWs) such as tasers are weapons used by law enforcement that deliver high-voltage current that is neither true AC or DC but is most like a series of low-amplitude DC shocks.[16] They can deliver 50,000 V in a 5-second pulse, with an average current of 2.1 mA.[17] Though they have been temporally associated with deaths in the law enforcement setting, conducted electrical devices (CEDs) in healthy volunteers have been shown to be safe without evidence of delayed arrhythmia or cardiac damage as measured by troponin I.[18, 17] One study of their use in 1201 law enforcement incidents showed mostly superficial puncture wounds from the device probes, and significant injuries only from trauma subsequent to shock, not from the device itself. Of 2 deaths in custody, neither was related to CEW exposure.[19]

stop gunshot wound bleeding in 15 seconds

Microsoft built a watch that helps people with Parkinson

People whose back or neck pain has not been relieved by back surgery or other treatments may have another option to consider: spinal cord stimulation. Around the world, some 14,000 patients undergo spinal cord stimulator implants each year. Spinal cord stimulation (SCS) delivers mild electrical stimulation to nerves along the spinal column, modifying or blocking nerve activity in a non-medicinal way to minimize the sensation of pain reaching the brain.
Ten percent of all pregnancies are complicated by hypertension. Eclampsia and preeclampsia account for about half of these cases worldwide, and these conditions have been recognized and described for years despite the general lack of understanding of the disease. [1] In the fifth century, Hippocrates noted that headaches, convulsions, and drowsiness were ominous signs associated with pregnancy. In 1619, Varandaeus coined the term eclampsia in a treatise on gynecology. [2, 3]
ormal sperm densities range from 15 million to greater than 200 million sperm per milliliter of semen. You are considered to have a low sperm count if you have fewer than 15 million sperm per milliliter or less than 39 million sperm total per ejaculate.

new study about the size of penis
