- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Intrauterine insemination (IUI) is a fertility treatment that involves placing sperm inside a woman's uterus to facilitate fertilization. The goal of IUI is to increase the number of sperm that reach the fallopian tubes and subsequently increase the chance of fertilization
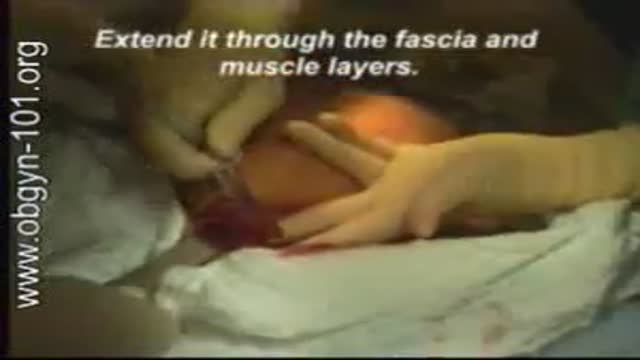
At one time, women who had delivered by cesarean section in the past would usually have another cesarean section for any future pregnancies. The rationale was that if allowed to labor, many of these women with a scar in their uterus would rupture the uterus along the weakness of the old scar. Over time, a number of observations have become apparent: Most women with a previous cesarean section can labor and deliver vaginally without rupturing their uterus. Some women who try this will, in fact, rupture their uterus. When the uterus ruptures, the rupture may have consequences ranging from near trivial to disastrous. It can be very difficult to diagnose a uterine rupture prior to observing fetal effects (eg, bradycardia). Once fetal effects are demonstrated, even a very fast reaction and nearly immediate delivery may not lead to a good outcome. The more cesarean sections the patient has, the greater the risk of subsequent rupture during labor. The greatest risk occurs following a “classical” cesarean section (in which the uterine incision extends up into the fundus.) The least risk of rupture is among women who had a low cervical transverse incision. Low vertical incisions probably increase the risk of rupture some, but usually not as much as a classical incision. Many studies have found the use of oxytocin to be associated with an increased risk of rupture, either because of the oxytocin itself, or perhaps because of the clinical circumstances under which it would be contemplated. Pain medication, including epidural anesthetic, has not resulted greater adverse outcome because of the theoretical risk of decreasing the attendant’s ability to detect rupture early. The greatest risk of rupture occurs during labor, but some of the ruptures occur prior to the onset of labor. This is particularly true of the classical incisions. Overall successful vaginal delivery rates following previous cesarean section are in the neighborhood of 70 This means that about 30of women undergoing a vaginal trial of labor will end up requiring a cesarean section. Those who undergo cesarean section (failed VBAC) after a lengthy labor will frequently have a longer recovery and greater risk of infection than had they undergone a scheduled cesarean section without labor. Women whose first cesarean was for failure to progress in labor are only somewhat less likely to be succesful in their quest for a VBAC than those with presumably non-recurring reasons for cesarean section. For these reasons, women with a prior cesarean section are counseled about their options for delivery with a subsequent pregnancy: Repeat Cesarean Section, or Vaginal Trial of Labor. They are usually advised of the approximate 70successful VBAC rate (modified for individual risk factors). They are counseled about the risk of uterine rupture (approximately 1in most series), and that while the majority of those ruptures do not lead to bad outcome, some of them do, including fetal brain damage and death, and maternal loss of future childbearing. They are advised of the usual surgical risks of infection, bleeding, anesthesia complications and surgical injury to adjacent structures. After counseling, many obstetricians leave the decision for a repeat cesarean or VBAC to the patient. Both approaches have risks and benefits, but they are different risks and different benefits. Fortunately, most repeat cesarean sections and most vaginal trials of labor go well, without any serious complications. For those choosing a trial of labor, close monitoring of mother and baby, with early detection of labor abnormalities and preparation for

Loyola Full Male Exam Part 4 A video from Loyola medical school, Chicago showing the full examination of the male

Remove a Plantar Wart from a foot Procedure
Traditional African treatment for infertility

Possible complications could include: Difficulty healing. Infection. Stump pain (severe pain in the remaining tissue) Phantom limb pain (a painful sensation that the foot or toe is still there) Continued spread of gangrene, requiring amputation of more areas of your foot, toes or leg. Bleeding. Nerve damage.

This video shows the delivery of the placenta after delivery of the fetus
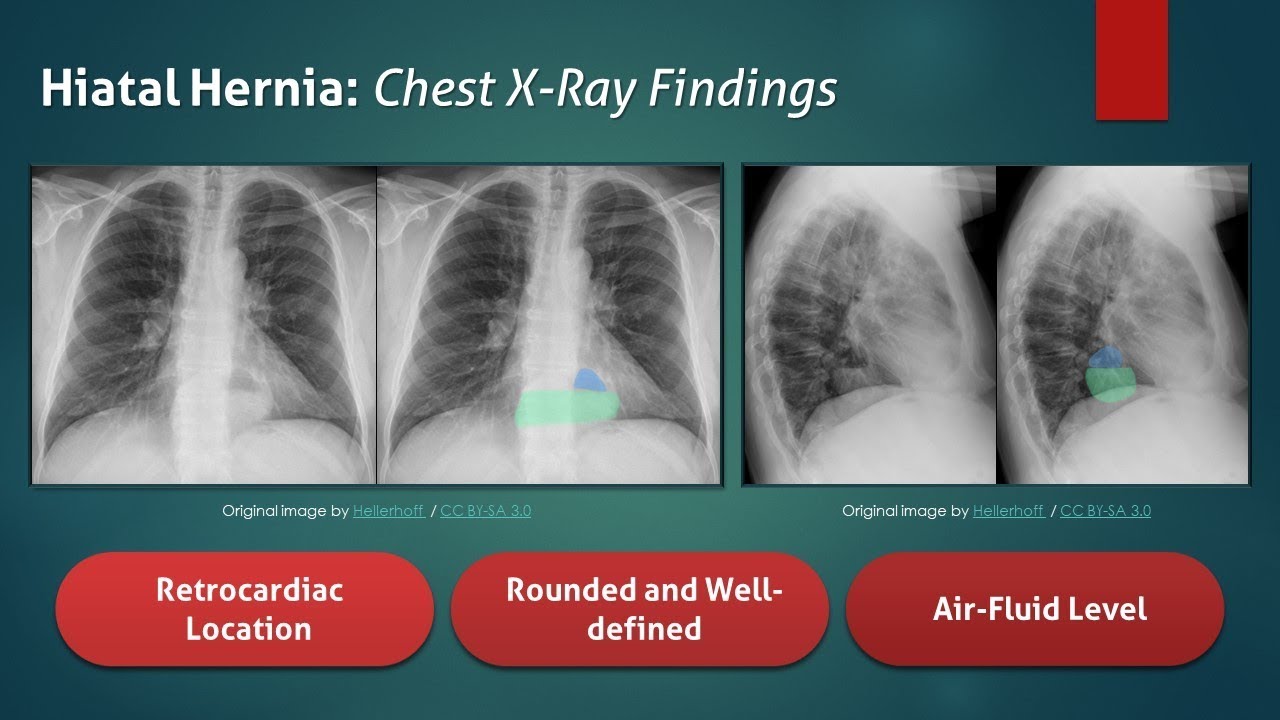
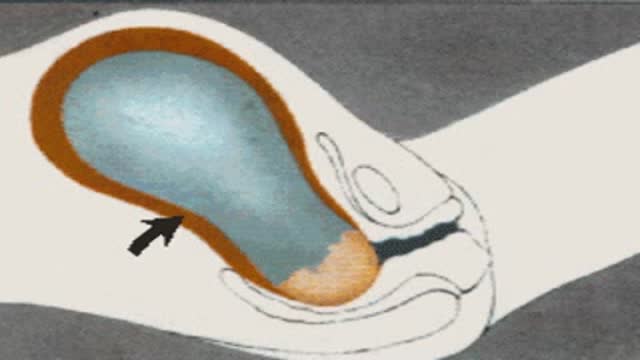
The typical radiograph is of a well-defined, rounded, retrocardiac opacity with an air-fluid level. In this image, the radiolucent gas is highlighted in blue, while the gastric contents are highlighted in the green. In many cases of hiatal hernia, there will not be an air bubble below the left hemidiaphragm. This is a relatively expected finding considering that the stomach is no longer in its usual position. The anatomical position of the herniated organ can be further elucidated on the lateral radiograph. Here we can see that the stomach is in the middle mediastinum posterior to the heart and above the diaphragm. Hiatal hernias can look similar to a retrocardiac lung abscess or another cavitary lesion, but it will change in size and shape between radiographs. Large hernias can shift the mediastinum to the right and result in a widening of the carinal angle. They can even give the appearance of cardiomegaly. In this radiograph, the cardiac silhouette is distinctly visible within the confines of the hiatal hernia. To review, a hiatal hernia on an AP chest radiograph typically appears as a round retrocardiac opacity with an air-fluid level.
🌐 Check out our website for more video lectures
https://www.med4vl.com
📺 Subscribe To My Channel and Get More Great Quizzes and Tutorials
https://www.youtube.com/channe....l/UC95TzSH1B_2EjaZMg
#FOAMrad #MedEd #radiology
Disclaimer: All the information provided by Medical Education for Visual Learners and associated videos are strictly for informational purposes only. It is not intended as a substitute for medical advice from your health care provider or physician. It should not be used to overrule the advice of a qualified healthcare provider, nor to provide advice for emergency medical treatment. If you think that you or someone that you know may be suffering from a medical condition, then please consult your physician or seek immediate medical attention.

The most common symptoms of infection from animal bites are redness, pain, swelling, and inflammation at the site of the bite. You should seek immediate medical treatment if any of these symptoms continue for more than 24 hours. Other symptoms of infection include: pus or fluid oozing from the wound

watch that Enema Insertion Medical Procedure
| MBBS मतलब JOHARI MBBS I
Download Johari MBBS APP ( For Online LIVE Classes, Notes, Books PDFs, Test Series )
Johari MBBS ( iPhone IOS Users ) LINK { FOR Online LIVE Classes }
https://apps.apple.com/in/app/....johari-mbbs/id647466
JOHARI MBBS APP ( Android ) LINK { FOR Online LIVE Classes }
https://play.google.com/store/....apps/details?id=co.d
CRASH COURSE LINK ( Anatomy in 30Days with Biochemistry In 7Days Series )
https://zczob.on-app.in/app/oc/389813/zczob
IMPORTANT LINKS :-
1) ORDER Anatomy Next Edition Module , Biochemistry in 7Days & Physiology MODULE
https://joharimbbs.com/
2) Join INSTAGRAM ( For Notes, Revision REELs, Updates )
https://www.instagram.com/johari_mbbs_lectures/
3) INSTA Broadcast Channel ( FOR Daily VLOGS, Life Update )
https://ig.me/j/Abal9xRcXcUyrYpT/
4) Telegram ( For FREE BOOKS PDFs )
https://t.me/joharimbbsofficial
5) Whatsapp Channel ( Daily Update )
https://whatsapp.com/channel/0....029VaEeWKWHAdNb0xOzl
6) Follow On Twitter ( For Latest Updates )
https://twitter.com/JohariMbbs
CRASH COURSE LINK ( Anatomy in 30Days with Biochemistry In 7Days Series )
https://zczob.on-app.in/app/oc/389813/zczob
#mbbs #joharimbbs #anaatomy #biochemistry #physiology #medico #doctors
histology slide identification tricks
histology slides identification tricks
histology slide
histology slides
histology slides identification
histology slide preparation
histology slides identification epithelium
histology slides identification connective tissue
histology slides identification tricks
histology slides of epithelium
histology slide identification
#anatomy#clinicalanatomy #MBBS #neroanatomy #bdc #medsudent #medicalcollege
For notes IG - johari_mbbs_lectures
link- https://www.instagram.com/p/CNOwFgEJmJL/
Join Telegram Channel ( JOhari MBBS Public 20x )
https://t.me/JohariMBBS
For Tag :-
histology , histology slides , histology slide identification , histology slides identification , histology slides preparation , tongue histology slide , histology slides asked in exam , histology slide identification trick , histology slides of connective tissue , mbbs histology , histology slides identification epithelium , trachea histology slide , slides , duodenum histology slide , histology slides tricks , histology slides review , examine histology slides

Butt implants are a popular plastic surgery procedure among those who wish to enhance the appearance, shape, and size of their rear ends. Buttock augmentation involves the surgical insertion of artificial body implants into a patient’s buttocks to create a larger, shapelier, and more sensuous rear end. Patients who have underdeveloped buttocks can achieve a more proportionate figure with butt implants. Women who wish to achieve an “hour glass” figure or are unhappy with the size of their buttocks can benefit from female butt implants. Men with flat or poorly developed buttocks can enhance the shape of the area to their liking with male butt implants. Many buttock augmentation patients say that their clothes fit better, they feel more attractive, and their confidence levels have improved.

Watch that video to know the Premature Ejaculation Causes and Cures

Genital warts are one of the most common types of sexually transmitted infections. At least half of all sexually active people will become infected with human papillomavirus (HPV), the virus that causes genital warts, at some point during their lives. Women are somewhat more likely than men to develop genital warts. As the name suggests, genital warts affect the moist tissues of the genital area. Genital warts may look like small, flesh-colored bumps or have a cauliflower-like appearance. In many cases, the warts are too small to be visible. Like warts that appear elsewhere on your body, genital warts are caused by the human papillomavirus (HPV). Some strains of genital HPV can cause genital warts, while others can cause cancer. Vaccines can help protect against certain strains of genital HPV

This video demonstrate Bilateral Salpingectomy for a patient suffering from hematosalpinx of one side and Hydrosalpinx other side in which one IVF has failed. Laparoscopic salpingectomy. In this less-invasive procedure, the surgeon makes 1-3 small incisions in the lower abdomen, and inserts a laparoscope into the pelvis through one of the incisions. The camera at the end of the laparoscope guides the surgeon through the procedure. The fallopian tube tissue is then removed. For more information https://www.laparoscopyhospital.com/
For more information please contact:
World Laparoscopy Hospital
Cyber City, Gurugram, NCR DELHI
INDIA 122002
Phone & WhatsApp: +919811416838, + 91 9999677788

This video demonstrates Laparoscopic Cholecystectomy Fully Explained Skin-to-Skin Video with Near Infrared Cholangiography performed by Dr R K Mishra at World Laparoscopy Hospital. A laparoscopic cholecystectomy is a minimally invasive surgical procedure that involves removing the gallbladder. It is typically performed using small incisions in the abdomen, through which a laparoscope (a thin tube with a camera and light) and surgical instruments are inserted. The surgeon uses the laparoscope to visualize the inside of the abdomen and to guide the instruments in removing the gallbladder.
Near-infrared cholangiography is a technique that uses a special camera and fluorescent dye to visualize the bile ducts during surgery. The dye is injected into the cystic duct (the tube that connects the gallbladder to the bile ducts) and the camera detects the fluorescence emitted by the dye, allowing the surgeon to see the bile ducts more clearly.
The combination of laparoscopic cholecystectomy and near-infrared cholangiography has become a standard of care in many hospitals and surgical centers. It allows for a more precise and efficient surgery, reducing the risk of complications such as bile duct injury.
The use of indocyanine green (ICG) with near-infrared imaging during laparoscopic cholecystectomy has several advantages. Here are some of them:
Better visualization of the biliary anatomy: ICG with near-infrared imaging allows for better visualization of the biliary anatomy during surgery. This helps the surgeon identify important structures, such as the cystic duct and the common bile duct, and avoid injuring them.
Reduced risk of bile duct injury: With better visualization of the biliary anatomy, the risk of bile duct injury during surgery is reduced. Bile duct injury is a serious complication that can occur during laparoscopic cholecystectomy and can lead to long-term health problems.
Improved surgical precision: ICG with near-infrared imaging also improves surgical precision. The surgeon can better see the tissues and structures being operated on, which can help reduce the risk of bleeding and other complications.
Shorter operating time: The use of ICG with near-infrared imaging can shorten the operating time for laparoscopic cholecystectomy. This is because the surgeon can more quickly and accurately identify the biliary anatomy, which can help streamline the surgery.
Overall, the use of ICG with near-infrared imaging is a valuable tool in laparoscopic cholecystectomy that can improve surgical outcomes and reduce the risk of complications.
Like any surgical procedure, laparoscopic cholecystectomy (gallbladder removal) has potential complications. Here are some of the most common ones:
Bleeding: Bleeding during or after the surgery is a possible complication of laparoscopic cholecystectomy. Most cases are minor and can be easily controlled, but in rare cases, significant bleeding may require a blood transfusion or even additional surgery.
Infection: Any surgical procedure carries a risk of infection. After laparoscopic cholecystectomy, there is a risk of infection at the site of the incisions or within the abdomen. Symptoms may include fever, pain, redness, or drainage from the incision sites.
Bile leakage: In some cases, a small amount of bile may leak from the bile ducts into the abdominal cavity after gallbladder removal. This can cause abdominal pain, fever, and sometimes requires further surgery or treatment.
Injury to nearby organs: During the surgery, there is a small risk of unintentional injury to nearby organs such as the liver, intestines, or bile ducts. This can cause additional complications and may require further treatment.
Adverse reactions to anesthesia: As with any surgery requiring general anesthesia, there is a small risk of adverse reactions to the anesthesia, such as an allergic reaction, respiratory problems, or heart complications.
Most patients recover without complications following a laparoscopic cholecystectomy, but it is important to discuss any concerns or questions with your surgeon beforehand.
Contact us
World Laparoscopy Hospital
Cyber City, Gurugram, NCR Delhi
INDIA : +919811416838
World Laparoscopy Training Institute
Bld.No: 27, DHCC, Dubai
UAE : +971525857874
World Laparoscopy Training Institute
8320 Inv Dr, Tallahassee, Florida
USA : +1 321 250 7653
Regenerate response
A video showing vaginal delivery

Vaginoplasty is any surgical procedure that results in the construction or reconstruction of the vagina. It is a type of genitoplasty. Pelvic organ prolapse is often treated with one or more surgeries to repair the vagina.

Visit our website to learn more about using Nucleus animations for patient engagement and content marketing: http://www.nucleushealth.com/?utm_source=youtube&utm_medium=video-description&utm_campaign=appendect-020615
This 3D medical animation depicts the surgical removal of the appendix (appendectomy) using laparoscopic instruments. The surgery animation begins by showing an inflamed appendix (appendicitis), followed by the placement of the laparoscope. Afterward, one can see the surgical device staple, cut and remove the inflamed appendix. Following the removal of the appendix the abdomen is flushed with a sterile saline solution to ensure all traces of infection have been removed.
#laparoscopy #appendix #appendicitis
ANCE00183
Brought to you by http://nursing-resource.com
