- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
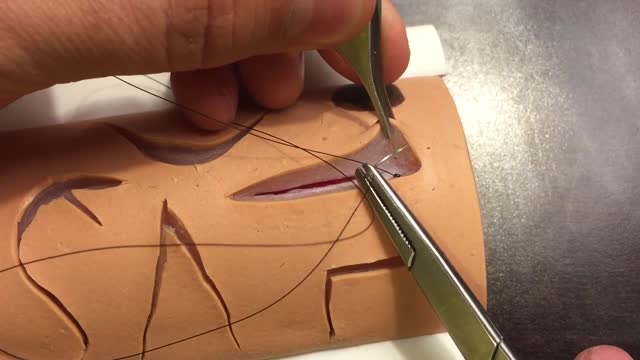
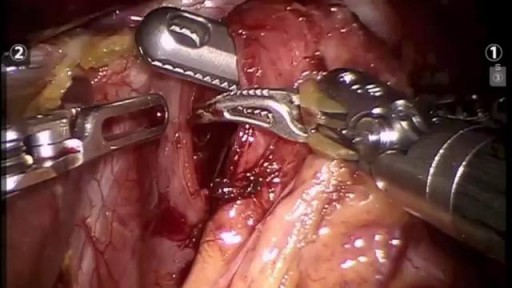
The two biggest considerations when choosing a suture are the location and tension of the wound. Other important considerations are tensile strength, knot strength, handling, and tissue reactivity. Sutures are divided into two major groups: Absorbable – lose the majority of their tensile strength in less than 60 days. They are generally used for buried sutures and do not require removal. Non-absorbable – maintain the majority of their tensile strength for more than 60 days. They are generally used for skin surface sutures and do require removal postoperatively. Suture needles also come in a variety of shapes and sizes. Curved needles are almost exclusively used in dermatological surgery. Cutting needles move through the tissue more easily and may have their primary cutting edge on the inside of the curve (conventional cutting) or outside of the curve (reverse cutting). The benefit of reverse cutting is that the tapered puncture left by the suture is directed away from the wound edge and therefore tissue tearing is less common. Non-cutting round needles cause even less tissue tearing and may be especially useful in delicate areas and fascia.
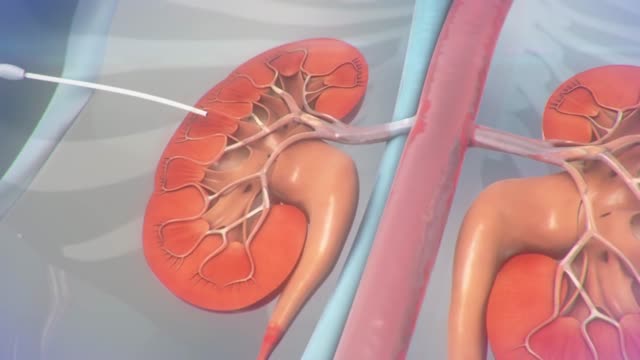
A ureteral stent is a thin, hollow tube that is placed in the ureter to help urine pass from the kidney into the bladder. Ureters are the tubes that connect the kidneys to the bladder. You may have a small amount of blood in your urine for 1 to 3 days after the procedure.
Overactive bladder syndrome is common. Symptoms include an urgent feeling to go to the toilet, going to the toilet frequently and sometimes leaking urine before you can get to the toilet (urge incontinence). Treatment with bladder training often cures the problem. Sometimes medication may be advised in addition to bladder training to relax the bladder.
A new Harvard study claims a breakthrough that could lead to a new treatment of Type 1 diabetes. WSJ's Ron Winslow explains what it means on Lunch Break. Photo: Getty
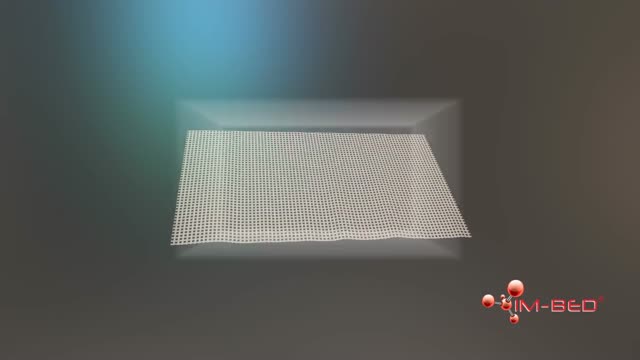
Wound healing is the process by which skin or other body tissue repairs itself after trauma. ... This process is divided into predictable phases: blood clotting (hemostasis), inflammation, tissue growth (proliferation) and tissue remodeling (maturation).
The cornea occupies the front center part of the outer wall of the eye. It is made of collagen fibers in a very special arrangement so that the cornea is clear. One looks through the cornea to see the iris and pupil. The cornea bends light coming into the eye so that it is focused on the retina.

INVIVO
The accumulation of ascitic fluid represents a state of total-body sodium and water excess, but the event that initiates the unbalance is unclear. Although many pathogenic processes have been implicated in the development of abdominal ascites, about 75% likely occur as a result of portal hypertension in the setting of liver cirrhosis, with the remainder due to infective, inflammatory, and infiltrative conditions. Three theories of ascites formation have been proposed: underfilling, overflow, and peripheral arterial vasodilation. The underfilling theory suggests that the primary abnormality is inappropriate sequestration of fluid within the splanchnic vascular bed due to portal hypertension and a consequent decrease in effective circulating blood volume. This activates the plasma renin, aldosterone, and sympathetic nervous system, resulting in renal sodium and water retention. The overflow theory suggests that the primary abnormality is inappropriate renal retention of sodium and water in the absence of volume depletion. This theory was developed in accordance with the observation that patients with cirrhosis have intravascular hypervolemia rather than hypovolemia. The most recent theory, the peripheral arterial vasodilation hypothesis, includes components of both of the other theories. It suggests that portal hypertension leads to vasodilation, which causes decreased effective arterial blood volume. As the natural history of the disease progresses, neurohumoral excitation increases, more renal sodium is retained, and plasma volume expands. This leads to overflow of fluid into the peritoneal cavity. The vasodilation theory proposes that underfilling is operative early and overflow is operative late in the natural history of cirrhosis. Although the sequence of events that occurs between the development of portal hypertension and renal sodium retention is not entirely clear, portal hypertension apparently leads to an increase in nitric oxide levels. Nitric oxide mediates splanchnic and peripheral vasodilation. Hepatic artery nitric oxide synthase activity is greater in patients with ascites than in those without ascites. Regardless of the initiating event, a number of factors contribute to the accumulation of fluid in the abdominal cavity. Elevated levels of epinephrine and norepinephrine are well-documented factors. Hypoalbuminemia and reduced plasma oncotic pressure favor the extravasation of fluid from the plasma to the peritoneal fluid, and, thus, ascites is infrequent in patients with cirrhosis unless both portal hypertension and hypoalbuminemia are present.
Obstetrics is the field of medicine which encompasses the care of a woman during pregnancy and childbirth. In that way it is very unique, as when assessing these patients, your actually also assessing another the child.
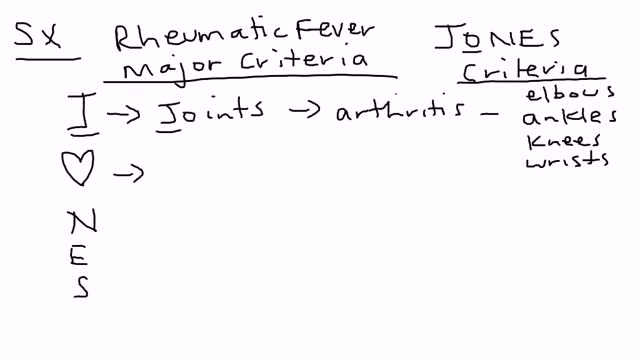
Rheumatic fever is an inflammatory disease that can develop as a complication of inadequately treated strep throat or scarlet fever. Strep throat and scarlet fever are caused by an infection with streptococcus bacteria. Rheumatic fever is most common in 5- to 15-year-old children, though it can develop in younger children and adults. Although strep throat is common, rheumatic fever is rare in the United States and other developed countries. However, rheumatic fever remains common in many developing nations. Rheumatic fever can cause permanent damage to the heart, including damaged heart valves and heart failure. Treatments can reduce damage from inflammation, lessen pain and other symptoms, and prevent the recurrence of rheumatic fever.

If it gets more severe and causes symptoms, your low hemoglobin count may indicate you have anemia. A low hemoglobin count is generally defined as less than 13.5 grams of hemoglobin per deciliter (135 grams per liter) of blood for men and less than 12 grams per deciliter (120 grams per liter) for women.
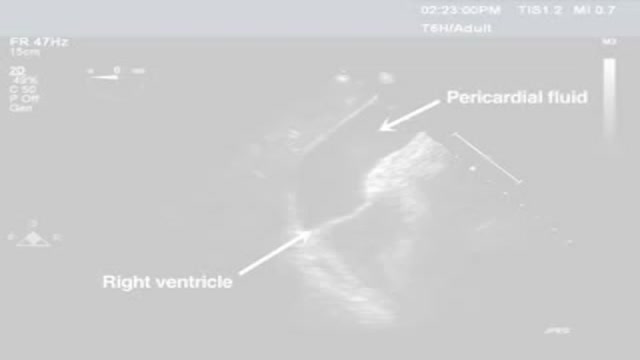
Pericardiocentesis is the aspiration of fluid from the pericardial space that surrounds the heart. This procedure can be life saving in patients with cardiac tamponade, even when it complicates acute type A aortic dissection and when cardiothoracic surgery is not available. [1] Cardiac tamponade is a time sensitive, life-threatening condition that requires prompt diagnosis and management. Historically, the diagnosis of cardiac tamponade has been based on clinical findings. Claude Beck, a cardiovascular surgeon, described 2 triads of clinical findings that he found associated with acute and chronic cardiac tamponade. The first of these triads consisted of hypotension, an increased venous pressure, and a quiet heart. It has come to be recognized as Beck's triad, a collection of findings most commonly produced by acute intrapericardial hemorrhage. Subsequent studies have shown that these classic findings are observed in only a minority of patients with cardiac tamponade. [2] The detection of pericardial fluid has been facilitated by the development and continued improvement of echocardiography. [3] Cardiac ultrasound is now accepted as the criterion standard imaging modality for the assessment of pericardial effusions and the dynamic findings consistent with cardiac tamponade. With echocardiography, the location of the effusion can be identified, the size can be estimated (small, medium, or large), and the hemodynamic effects can be examined by assessing for abnormal septal motion, right atrial or right ventricular inversion, and decreased respiratory variation of the diameter of the inferior vena cava.
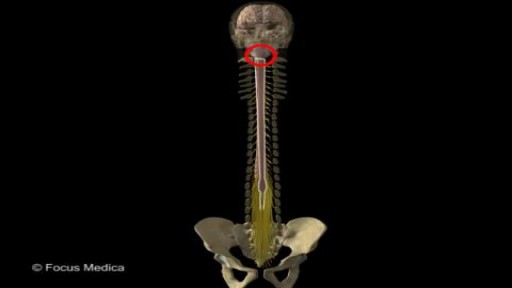
Back and Spinal cord Anatomy

Both selegiline and rasagiline can improve the symptoms of Parkinson's disease, although their effects are small compared with levodopa. They can be used alongside levodopa or dopamine agonists. MAO-B inhibitors are generally very well tolerated, but can occasionally cause side effects, including: nausea.

ADC was first identified early in the AIDS epidemic as a common and novel CNS syndrome.(4,5) The three components of the term, AIDS dementia complex embody central features of the condition. AIDS emphasizes its morbidity and poor prognosis, particularly when its severity is at stage 2 or greater (see Table 1), a severity comparable to other clinical AIDS-defining complications of HIV-1 infection. Dementia designates the acquired and persistent cognitive decline with preserved alertness that usually dominates the clinical presentation and determines its principal disability. Complex emphasizes that this disease not only impairs the intellect, but also concomitantly alters motor performance and, at times, behavior. This involvement of the nervous system beyond cognition is evidence of a wider involvement of the CNS than occurs in some other types of dementia such as Alzheimer's disease. Additionally, myelopathy may be an important, indeed predominating, aspect of ADC, and organic psychosis may also be a feature in a subset of patients (see Rheumatologic and Musculoskeletal Manifestations of HIV). These manifestations are therefore also encompassed within this term. By contrast, neither neuropathy nor functional psychiatric disturbance are included in ADC.
Eosinophilic granulomatosis with polyangiitis (EGPA; also known as Churg-Strauss syndrome [CSS] or allergic granulomatosis) is a rare autoimmune condition that causes inflammation of small and medium-sized blood vessels (vasculitis) in persons with a history of airway allergic hypersensitivity (atopy).

Preparing The Kidney for Transplant
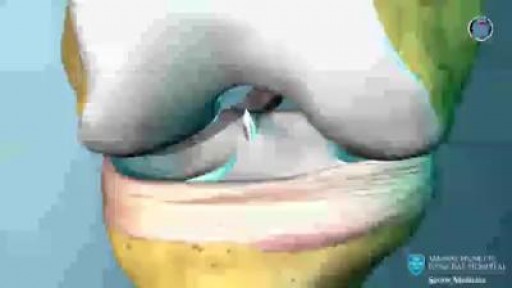
In nonsurgical treatment, progressive physical therapy and rehabilitation can restore the knee to a condition close to its pre-injury state and educate the patient on how to prevent instability.37, 38 This may be supplemented with the use of a hinged knee brace. However, many people who choose not to have surgery may experience secondary injury to the knee due to repetitive instability episodes. Surgical treatment is usually advised in dealing with combined injuries (ACL tears in combination with other injuries in the knee). However, deciding against surgery is reasonable for select patients. Nonsurgical management of isolated ACL tears is likely to be successful or may be indicated in patients:
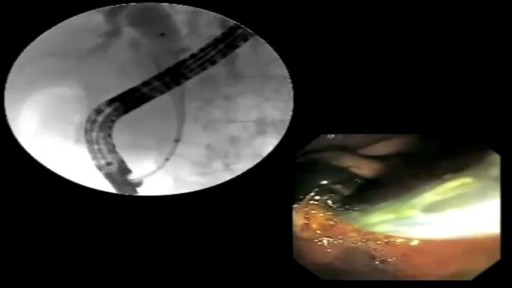
The placement of a percutaneous expandable biliary endoprosthesis was first reported in 1985 by Carrasco et al. in a canine model,[1] and the endoscopic placement of expandable metal stents to relieve biliary strictures in patients was first described in 1989.[2,3] Over the past two decades, the endoscopic approach to biliary endoprosthesis placement has largely supplanted the percutaneous approach. Self-expanding metal stents (SEMS) have traditionally been used for palliation of obstructive jaundice in patients with unresectable pancreaticobiliary tumors. However, SEMS are increasingly being used in patients with resectable cancers[4] and benign biliary strictures.[5] Uncovered SEMS (uSEMS) have been shown to have longer patency periods than plastic stents when used for malignant biliary obstruction and to be cost effective if the patient's life expectancy is greater than 4–6 months.[6–8] The common causes of malignant biliary obstruction are pancreatic cancer and cholangiocarcinoma.[9–11] Biliary drainage prior to surgical resection is controversial; several investigators have reported it to be beneficial owing to the improved tissue healing with reduced bilirubin levels,[12,13] but others have also reported its deleterious effects secondary to the additional intervention..
