- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
The epididymis is a long coiled tube that lies above and behind each testicle. The epididymis collects and transports sperm from the testis to the vas deferens (tubes that transport sperm to the urethra). An epididymal cyst is a cyst-like mass in the epididymis that contains clear fluid. Typically, epididymal cysts and spermatoceles do not cause symptoms. When discovered, the epididymal cyst is usually about the size of a pea and feels separate from the top of the testis. Spermatoceles typically arise from the head of the epididymis, and are felt on the top portion of the testicle. Epididymal cysts and spermatoceles are often incidental findings on testicular self-examination or routine physical examination. It is important that any mass noted in the scrotum be examined by a urologist in order to obtain an accurate diagnosis, especially a mass on the testicle itself. Our team in the Division of Urology will typically be able to confirm the diagnosis on physical exam. However, a scrotal ultrasound may also be used in order to rule out other conditions.

Gallstone ileus is an important, though infrequent, cause of mechanical bowel obstruction, affecting older adult patients who often have other significant medical conditions. It is caused by impaction of a gallstone in the ileum after being passed through a biliary-enteric fistula. The diagnosis is often delayed since symptoms may be intermittent and investigations fail to identify the cause of the obstruction. The mainstay of treatment is removal of the obstructing stone after resuscitating the patient. Gallstone ileus continues to be associated with relatively high rates of morbidity and mortality.

A thyroid biopsy is a procedure in which a small sample of tissue is removed from the thyroid gland and looked at under a microscope for cancer, infection, or other thyroid problems. The thyroid gland is found in front of the windpipe (trachea), just below the voice box (larynx). A sample of thyroid tissue can be taken by: Fine-needle biopsy. Your doctor puts a thin needle through the skin and into the thyroid gland. Many thyroid specialists like to use a needle biopsy method rather than surgery. Open biopsy. Your doctor makes a cut (incision) through the skin to see the thyroid gland. This method is done when other tests have not found the cause of your symptoms. Core needle biopsy. Your doctor inserts a needle with a special tip and removes a sample of tissue about the size of a grain of rice.
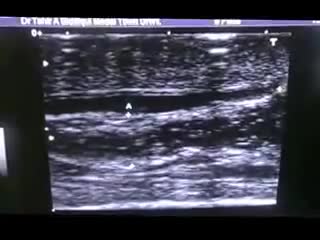
A central venous catheter, also called a central line, is a long, thin, flexible tube used to give medicines, fluids, nutrients, or blood products over a long period of time, usually several weeks or more. A catheter is often inserted in the arm or chest through the skin into a large vein.

A biopsy is a diagnostic test that involves collecting small pieces of tissue, usually through a needle, for examination with a microscope. A kidney biopsy can help in forming a diagnosis and in choosing the best course of treatment.


10 Animals Found Living Inside Humans

A 76 year-old, female, presented with a three day history of melena without any abdominal pain. She had one episode of hematemesis (about 100 ml blood) in the emergency room, patient has a strong alcoholic drink abuse.
An upper endoscopy with magnification was performed.
multiple ulcers were detected across of the gastric camera,
esophageal varices was also detected

-Tibial stress fractures are common in athletes and nonathletes who suddenly increase their physical activity. Clinical features include pain, localized tenderness, and swelling. Plain x-ray is <50% sensitive for stress fractures, especially in the first 2-3 weeks after the onset of symptoms. MRI is preferred over bone scan or ultrasound as it can show the fracture line that extends through the cortex into the medullary line. MRI can also identify ligament, muscle, and cartilage injuries. However, MRI findings may be persistently abnormal for up to 1 year after the stress fracture has healed.

Tracheostomy


Dr. Nick demonstrates how easy it is to have stitches taken out and that it is not painful!
#shorts #satisfying #reaction
 MAKE SURE TO SUBSCRIBE FOR ALL THE NEW SURGICAL AND EDUCATIONAL VIDEOS COMING!!
👉🏻For more information visit :
https://drnickcampi.com
👉🏻Follow me on TikTok!!
https://vm.tiktok.com/ZMeXLbc5F/
👉🏻Connect with me!!
https://www.instagram.com/drnickcampitelli
👉🏻Check out this video of how we remove an ingrown toenail!
https://youtu.be/JyZo8aZDYds
👉🏻Dr. Nick Campitelli Performs latest Minimally Invasive Bunion Surgery! Watch this video!
https://youtu.be/eRpABMsCbOU
Dr. Nick Campitelli is a podiatrist who specializes in foot and ankle surgery in the Akron and Cleveland Ohio area. He is the Residency Director of the Western Reserve Hospital / University Hospital Podiatric Medicine and Surgery Residency Program.
*** All content found on the this YouTube video including: text, images, audio, or other formats were created for informational purposes only. The Content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you heard on this video. ***

.

Each month inside your ovaries, a group of eggs starts to grow in small, fluid-filled sacs called follicles. Eventually, one of the eggs erupts from the follicle (ovulation). It usually happens about 2 weeks before your next period. Hormones Rise After the egg leaves the follicle, the follicle develops into something called the corpus luteum. The corpus luteum releases a hormone that helps thicken the lining of your uterus, getting it ready for the egg. The Egg Travels to the Fallopian Tube After the egg is released, it moves into the Fallopian tube. It stays there for about 24 hours, waiting for a single sperm to fertilize it. All this happens, on average, about 2 weeks after your last period.
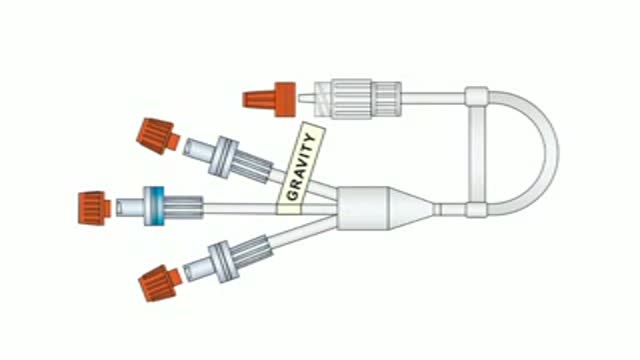
To facilitate the delivery of fluids during labour, obstetric anaesthetists from Coventry designed a triple IV peripheral connector with a central high-flow anti-reflux valve. This connector, now rightly known as the Coventry valve, can be used for all theatre settings and is especially useful in obstetrics, ICU, HDU and orthopaedics. More details on www.mediplus.co.uk

A Beautiful Smile at Lake Pointe is Sugar Land premier dentistry practice. Dr. Lance Jue has been serving patients' preventive, restorative and cosmetic dental needs here in Sugar Land for over 19 years. Book an appointment online now with Dr. Lance Jue

Parasitic Worm removed from Man's EYE


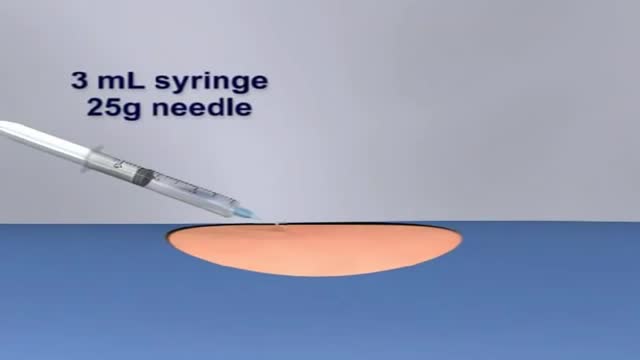
This video demonstrates the process for preparing and administering an intramuscular injection (IM)
A talus fracture is a break in one of the bones that forms the ankle. This type of fracture often occurs during a high-energy event, such as a car collision or a high-velocity fall. Because the talus is important for ankle movement, a fracture often results in significant loss of motion and function. In addition, a talus fracture that does not heal properly can lead to serious complications, including chronic pain. For this reason, many talus fractures require surgery.
