- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Loyola Respiratory System Exam Part 1 A video from Loyola Medical School, Chicago showing the medical and clinical examination of the respiratory system.
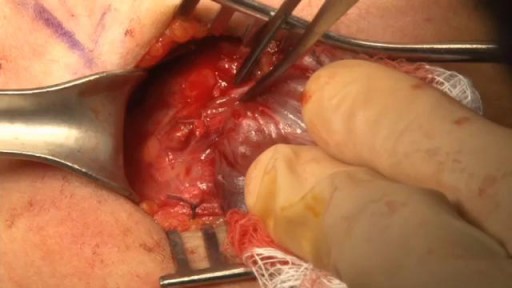
Lembert Pattern Suture

The period between stages one and two of labour

Female condoms are easy to use with a little practice. Here are the basics on how to insert, use, and remove a female condom.
Demonstration of Ballon Stent Surgery

secret about human

Ingrown hair removal on thigh #18

Microsurgical resection of Vocal fold polyp

This membrane could prevent heart attacks and keep the heart alive.

A few words on connective tissue. Please see disclaimer on my website www.academyofprofessionals.com

Polycystic ovary syndrome (PCOS, also known clinically as Stein-Leventhal syndrome), which is an endocrine disorder that affects 5--10% of women. It occurs amongst all races and nationalities, is the most common hormonal disorder among women of reproductive age, and is a leading cause of infertility. The symptoms and severity of the syndrome vary greatly between women. While the causes are unknown, insulin resistance (often secondary to obesity) is heavily correlated with PCOS.

A 76 year-old, female, presented with a three day history of melena without any abdominal pain. She had one episode of hematemesis (about 100 ml blood) in the emergency room, patient has a strong alcoholic drink abuse.
An upper endoscopy with magnification was performed.
multiple ulcers were detected across of the gastric camera,
esophageal varices was also detected

Henry Anhalt DO FAAP
Ped Eddo

Soft tissue biopsy from osteolytic lesions is a challenge for the interventionist. The Spirotome Bone is conceived for this intervention. The procedure is straigthforward and produces tissue specimens of high quality in sufficient amounts to allow quantitative molecular biology.

Ganglion Cyst Surgical Removal

Ear Weber's Test from the USMLE collection

Pulmonary Artery
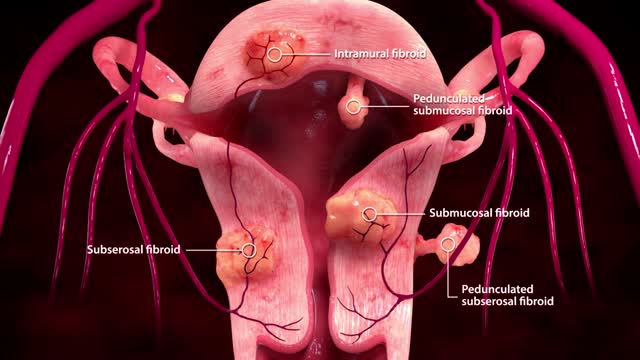
Uterine fibroid embolization (UFE), also known as uterine artery embolization, is a minimally invasive procedure that is performed by an Interventional Radiologist (IR), a doctor who uses advanced imaging technology to see inside the body without surgery. UFE is often performed as an outpatient service and offers a much shorter recovery time than surgery. For more information on uterine fibroids and all your treatment options, including UFE,
Watch that Thyroid Removal Surgery

DMC Children's Hospital of Michigan -- where everything we do is just for them. ~ Detroit Medical Center
