- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

brain surgery Blood Clot, removal of blood clot in brain, hematoma brain surgery

Follow these steps for a successful home extraction: Clean your hands. Wash your hands with soap and warm water. ... Clean your face. Wash and gently exfoliate your face. ... Sterilize your tools. ... Sterilize the pimple. ... Pierce the pimple. ... Create a small tear. ... Release the pus. ... Apply drying lotion

Dr. Arthur Handal explains the differences patients can expect when their surgeon chooses to use either a needle or a cannula to inject facial fillers.


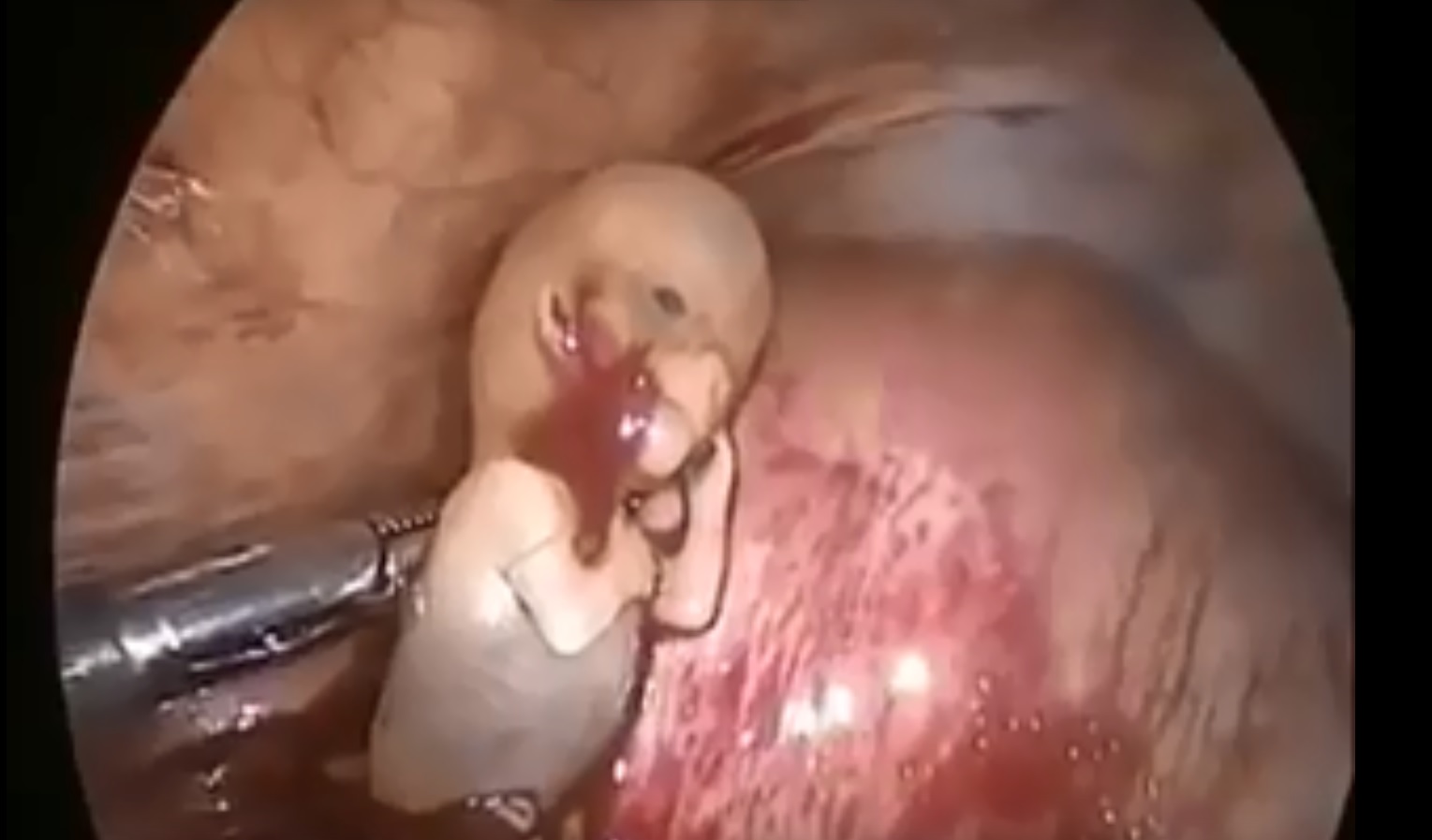
Watch that Ectopic Baby Removal Surgery

Most scoliosis surgeons agree that children who have very severe curves (45-50° and higher) will need surgery to lessen the curve and prevent it from getting worse. The operation for scoliosis is a spinal fusion. The basic idea is to realign and fuse together the curved vertebrae so that they heal into a single, solid bone. With the tools and technology available today, scoliosis surgeons are able to improve curves significantly.
Because of his weight, Jimmie Jones was on the waiting list for a new kidney for 17 years. University of Illinois Hospital surgeons used robotic surgery to give him a life without dialysis.
Best Gynecomastia surgeon in India is Dr. Ajaya Kashyap, with over 20 years experience in breast surgeries. He is the only active Indian member in American Society of Plastic Surgeons. Contact us to find out about your gynecomastia treatment in Delhi, India, maintaining high international standards, having a U.S. board certified surgeon, and latest technology and surgical techniques, our offices offer very economical costing. Contact us today inquire about gynecomastia surgery cost, in Delhi. You are sent query using WhatsApp and website.
For further information, are available visit our website: http://www.bestgynecomastiaindia.com/
Your Query for Chat and call +91-9818369662, 9958221983 (WhatsApp)
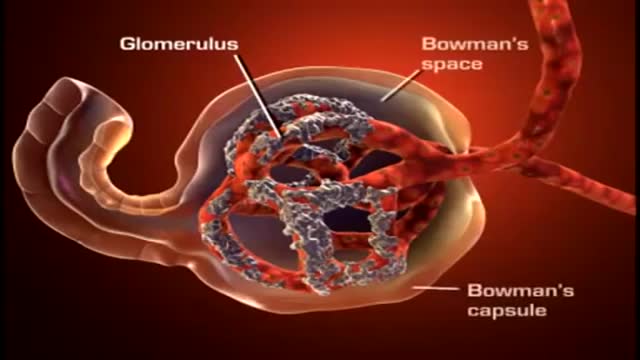
A nephron (from Greek νεφρός (nephros) meaning "kidney") is the basic structural and functional unit of the kidney. Its chief function is to regulate the concentration of water and soluble substances like sodium salts by filtering the blood, reabsorbing what is needed and excreting the rest as urine.

Download Clash of Clans for free for mobile devices. http://supr.cl/ThisArmy
I don't know you, BigBuffetBoy85
But if you think you can humiliate me and take my gold, think again.
Oh, I am coming for you with lots of Barbarians and Dragons. I can't wait to destroy your village, while you beg for mercy, but you will get no mercy. I will have my revenge.

An amputation is the removal of an extremity or appendage from the body. Amputations in the upper extremity can occur as a result of trauma, or they can be performed in the treatment of congenital or acquired conditions. Although successful replantation represents a technical triumph to the surgeon, the patient's best interests should direct the treatment of amputations. The goals involved in the treatment of amputations of the upper extremity include the following : Preservation of functional length Durable coverage Preservation of useful sensibility Prevention of symptomatic neuromas Prevention of adjacent joint contractures Early return to work Early prosthetic fitting These goals apply differently to different levels of amputation. Treatment of amputations can be challenging and rewarding. It is imperative that the surgeon treat the patient with the ultimate goal of optimizing function and rehabilitation and not become absorbed in the enthusiasm of the technical challenge of the replantation, which could result in poorer outcome and greater financial cost due to lost wages, hospitalization, and therapy.

Soon enough, a robot will be doing surgeries on you!
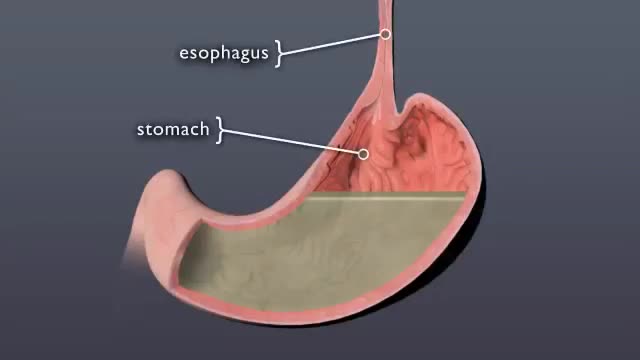
Discover what happens to pill when it swallowed

This is the incredible moment a new-born baby arrived still inside its amniotic sac, completely intact. The tiny infant can be seen moving and stretching still inside the sac, as medics prepare to snip the new born free. The amniotic sac is a thin but durable membrane filled with fluid which helps keep a baby warm and safe from bumps during pregnancy. When it breaks, this is typically referred to as a woman's 'waters breaking' shortly before she gives birth. But in rare cases, less than 1-in-80,000 births, the baby is delivered with the membranes still intact and this is known as a 'caul birth'. Some babies are born with part of the membrane still attached to them, but to be born completely encased in the intact membrane is incredibly rare. Many people still believe the phenomenon to be a good omen for the child's infancy and it is has even been suggested, but not proven, that caul babies will always have a natural affinity for water. The video was taken in Spain on Saturday and captures the rare moment the baby was born with the membrane covering its entire body, just minutes after its twin was delivered normally.

watch that Enema Insertion Medical Procedure

Watch that video to know Steroids Side Effects on The Human Body

Retinitis pigmentosa is a rare, inherited degenerative eye disease that causes severe vision impairment. Symptoms often begin in childhood. They include decreased vision at night or in low light and loss of side vision (tunnel vision).

The major elements of the cardiac exam include observation, palpation and, most importantly, auscultation (percussion is omitted). As with all other areas of the physical exam, establishing adequate exposure and a quiet environment are critical. Initially, the patient should rest supine with the upper body elevated 30 to 45 degrees. Most exam tables have an adjustable top. If not, use 2 or 3 pillows. Remember that although assessment of pulse and blood pressure are discussed in the vital signs section they are actually important elements of the cardiac exam.

Watch that Full Human Body Decay Process Video
