Toppvideor

Knee reflex video from the USMLE collection

What is inside A Cyst? Watch it now

Breast abscesses are often linked to mastitis – a condition that causes breast pain and swelling (inflammation), and usually affects women who are breastfeeding. Infections can occur during breastfeeding if bacteria enter your breast tissue, or if the milk ducts (tiny tubes) become blocked. This can cause mastitis which, if not treated, can result in an abscess forming. Women who aren't breastfeeding can also develop mastitis if bacteria enter the milk ducts through a sore or cracked nipple, or a nipple piercing. White blood cells are sent to attack the infection, which causes tissue at the site of the infection to die. This creates a small, hollow area that fills with pus (an abscess).

Laparoscopic treatment for Biliary Atresia. Kasai porto-enterostomy
Lumbar Laminotomy and Microdiscectomy

McMaster University technique of Laparoscopic Radical Nephrectomy

49-years old patient complaining of cough, fever and pleuritic pain for 2 weeks. At admission he was febrile and tachypnic. Chest X-Ray showed left pleural effusion. Thoracocentesis revealed purulent fluid. Chest CT-scan showed large and loculated left pleural effusion and pleural thickening. VATS decortication was performed through three incisions.

Epidermoid cysts, also called sebaceous, keratin, or epithelial cysts, are small, hard lumps that develop under the skin. These cysts are common. They grow slowly. They do not cause other symptoms and are nearly never cancerous. Epidermoid cysts are often found on the face, head, neck, back, or genitals
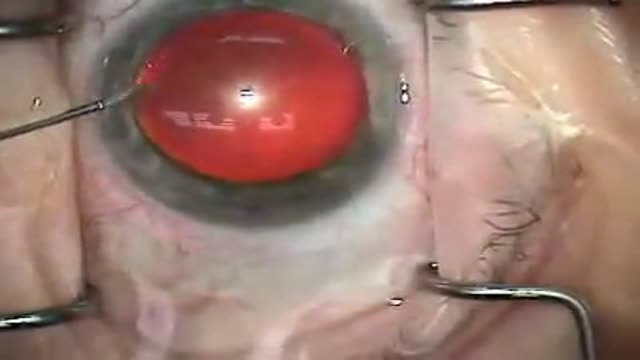
A video of modern cataract surgery employing a temporal, clear-corneal approach with topical anesthesia and ultrasound phacoemulsification; an aspheric silicone lens implant is inserted

A video showing the laser eye surgery

A very funny video

Spina bifida is a condition that affects the spine and is usually apparent at birth. It is a type of neural tube defect (NTD). Spina bifida can happen anywhere along the spine if the neural tube does not close all the way. When the neural tube doesn’t close all the way, the backbone that protects the spinal cord doesn’t form and close as it should. This often results in damage to the spinal cord and nerves. Spina bifida might cause physical and intellectual disabilities that range from mild to severe. The severity depends on: The size and location of the opening in the spine. Whether part of the spinal cord and nerves are affected.

Headaches with eating Ice Cream explained by medicine
The procedure of Suprapubic Cystostomy

Open Inguinal Hernia Repair Surgery - German Narration
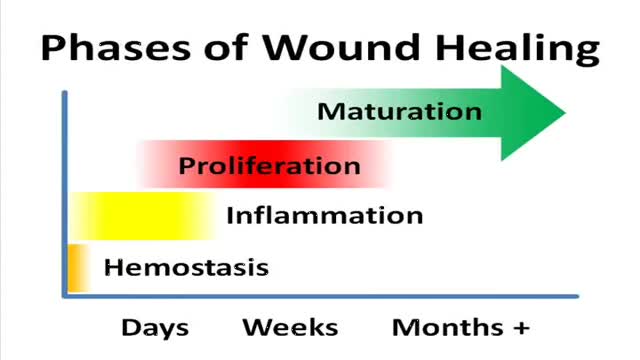
A video showing the phases of normal wound healing

A parasitic twin (also known as an asymmetrical or unequal conjoined twin) is the result of the processes that produce vanishing twins and conjoined twins, and may represent a continuum between the two. Parasitic twins occur when a twin embryo begins developing in utero, but the pair does not fully separate, and one embryo maintains dominant development at the expense of the other. Unlike conjoined twins, one ceases development during gestation and is vestigial to a mostly fully-formed, otherwise healthy individual twin. The undeveloped twin is defined as parasitic, rather than conjoined, because it is incompletely formed or wholly dependent on the body functions of the complete fetus. The independent twin is called the autosite.
Recently a group of affected females from Cameroon has started raising the voices against an old cultural "Female Abuse" tradition which is "Breast Ironing". The point of this tradition is to inhibit the growth of the female breast so that they will avoid getting raped.

How to open a glass ampoule

Doctors trying to reanimate a newborn after delivery.Watch till the end to see what happened..
